
Intra-Articular Injection of Cross-Linked Hyaluronic Acid-Dexamethasone Hydrogel Attenuates Osteoarthritis: An Experimental Study in a Rat Model of Osteoarthritis

 ,
,
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Results
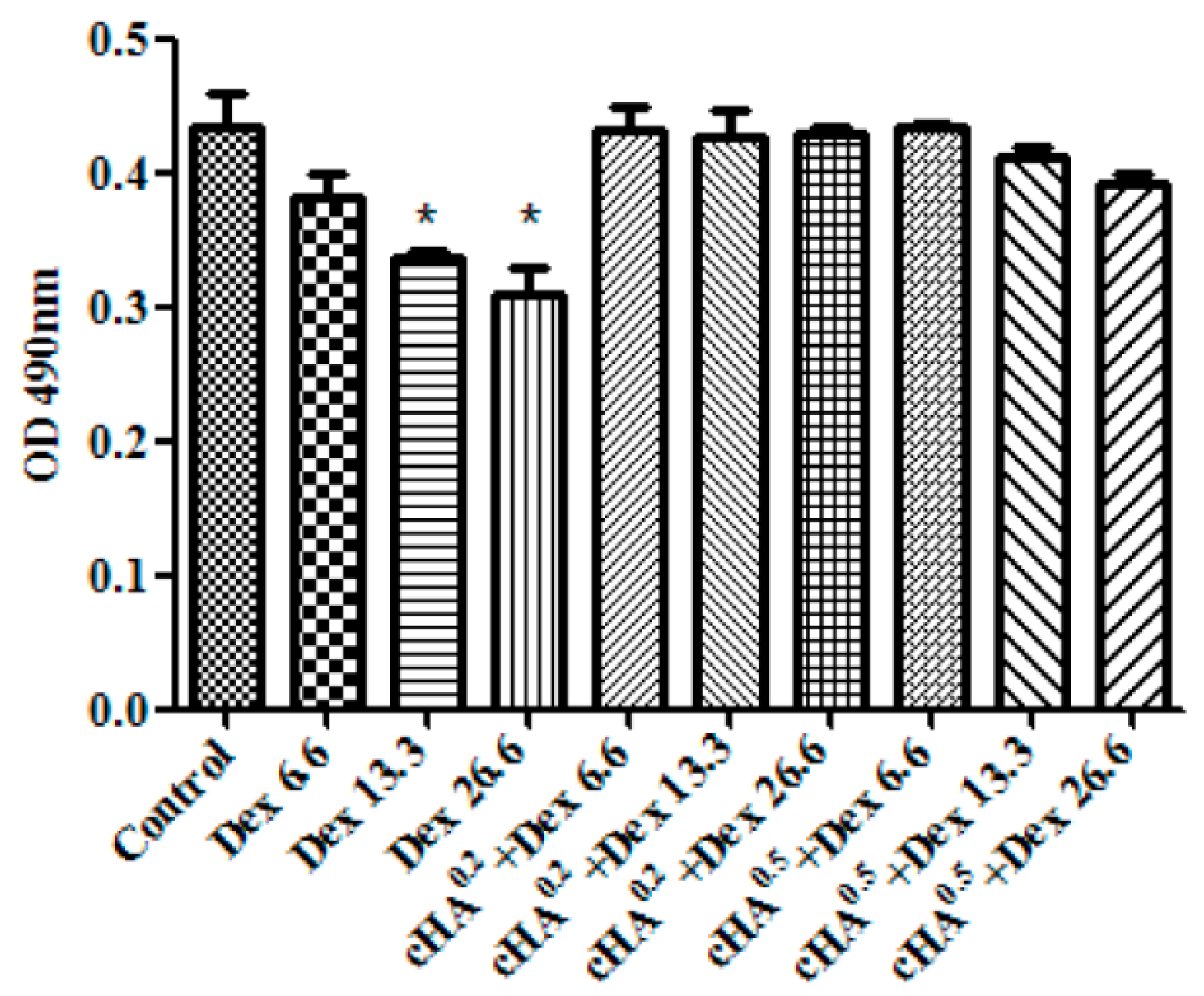
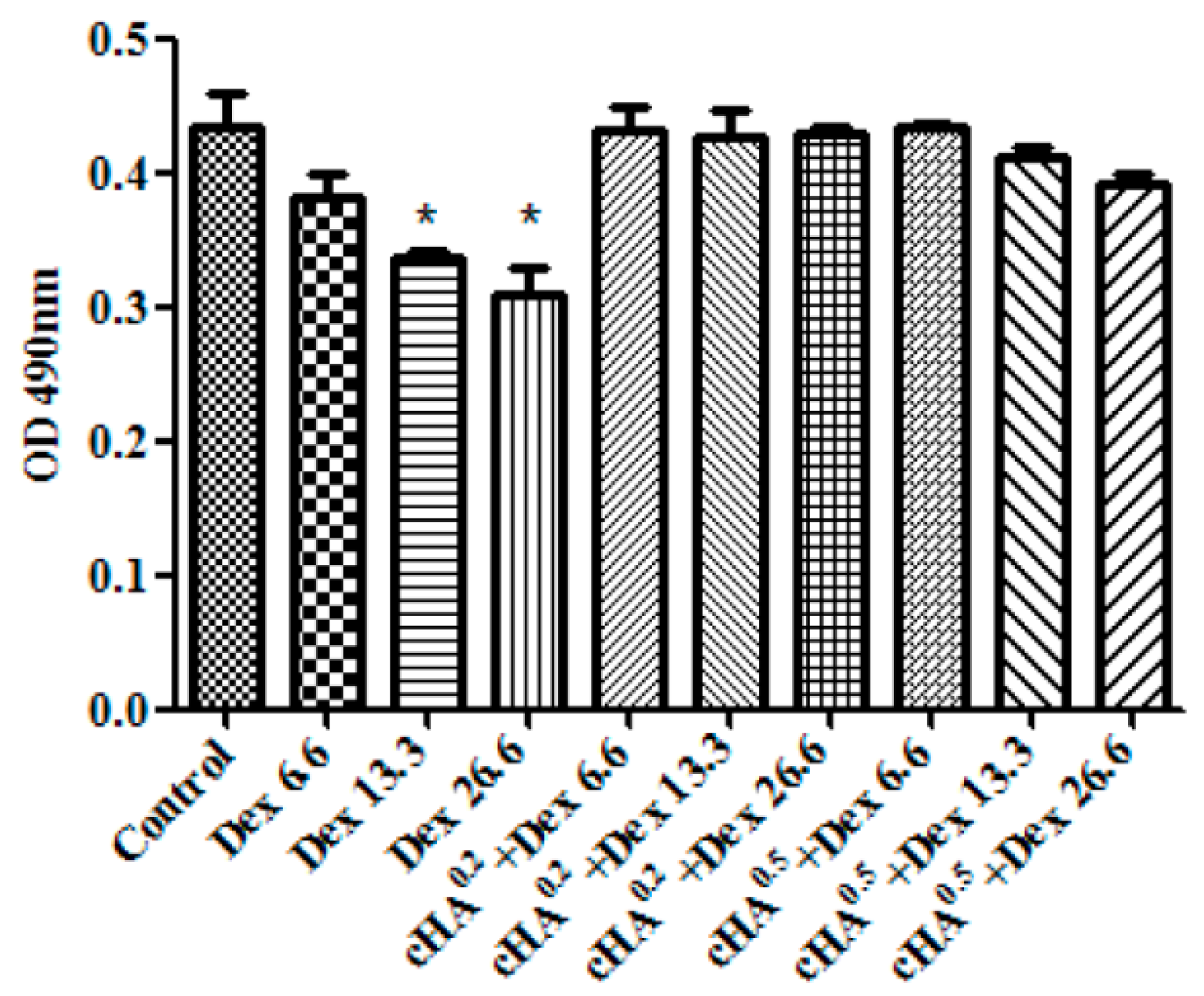
2.1. Cross-Linked Hyaluronic Acid-Dexamethasone (cHA-Dex) Hydrogel Exhibited Low Cytotoxicity in Vitro Compared with Dex Alone
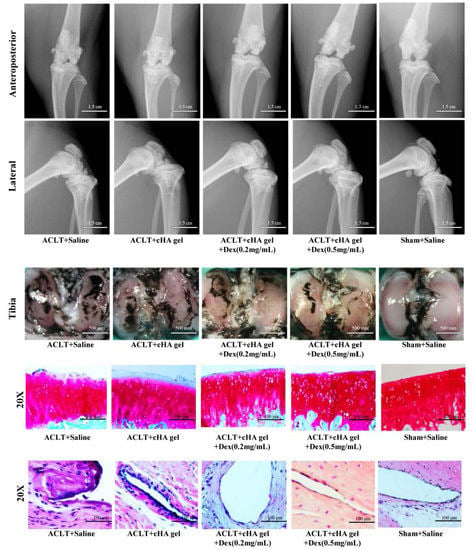
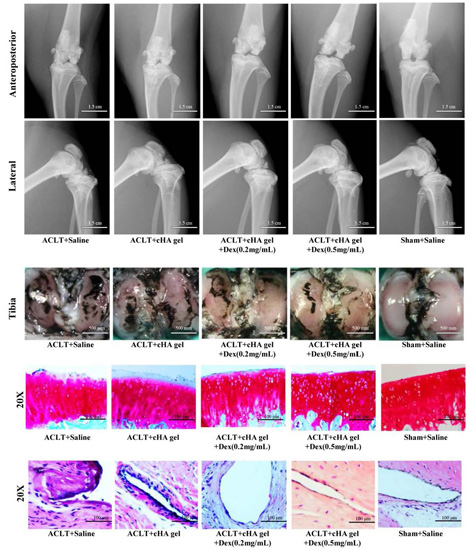
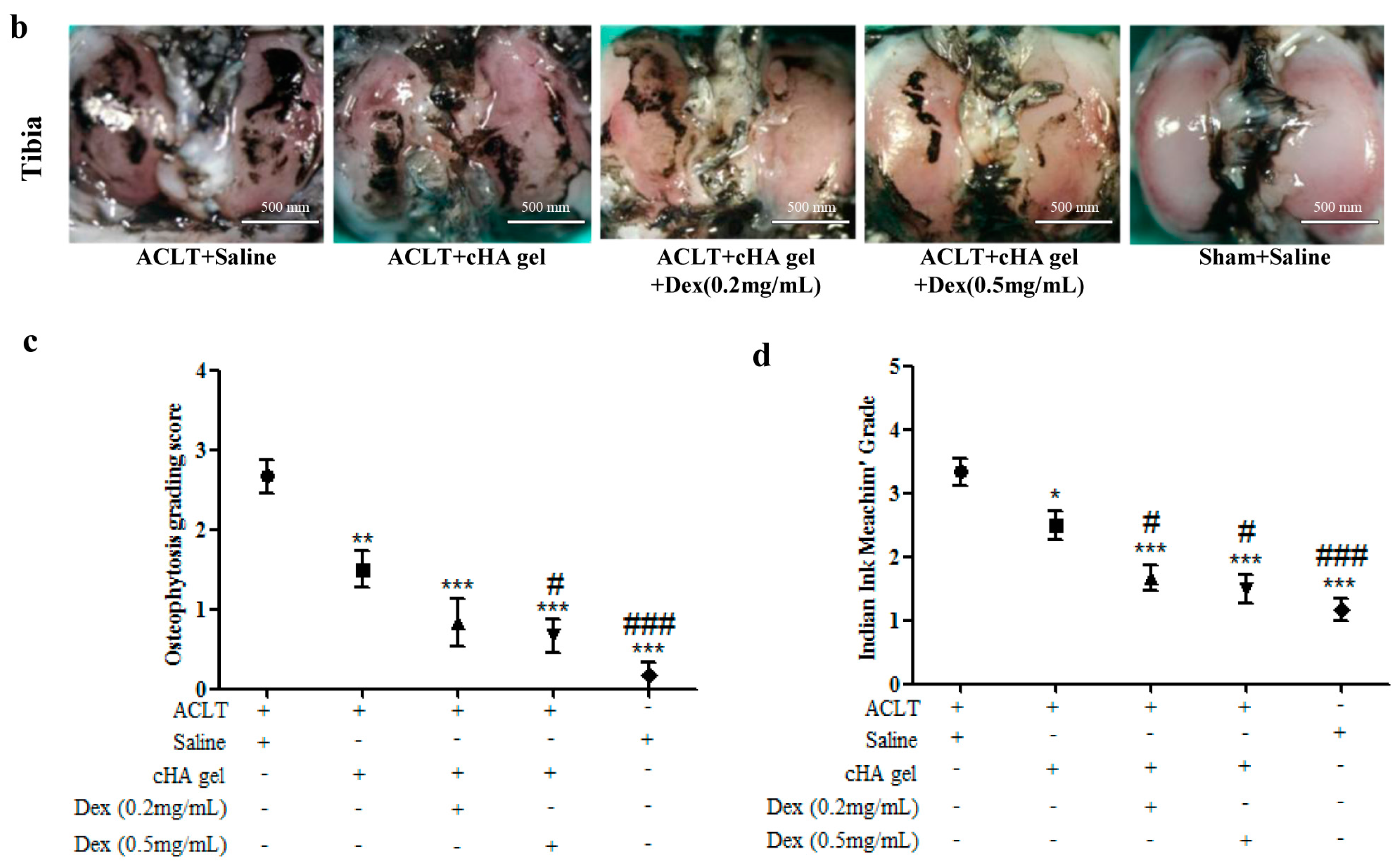
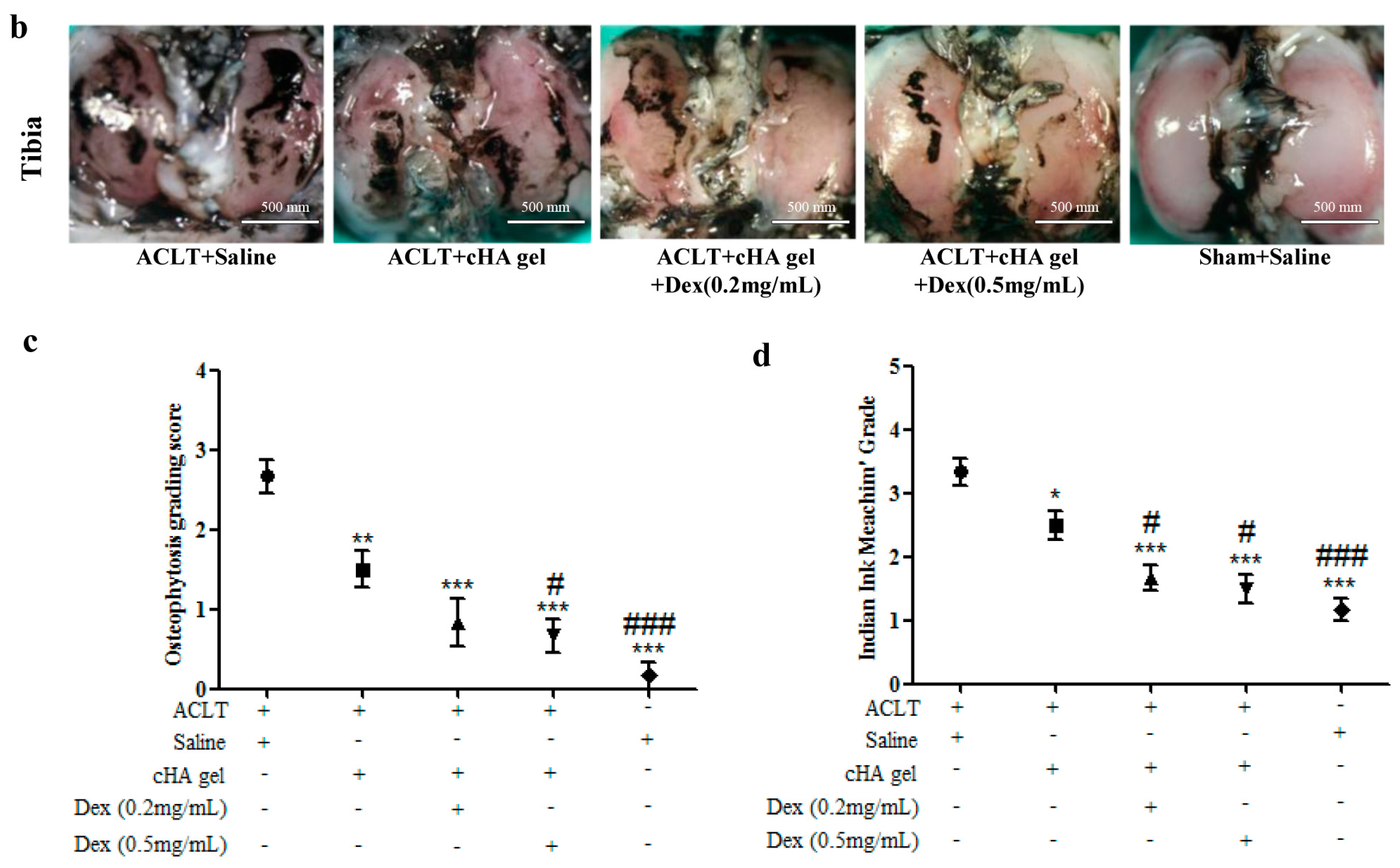
2.2. Intra-Articular cHA-Dex Hydrogel Injection Attenuated Osteoarthritis (OA) Macroscopically
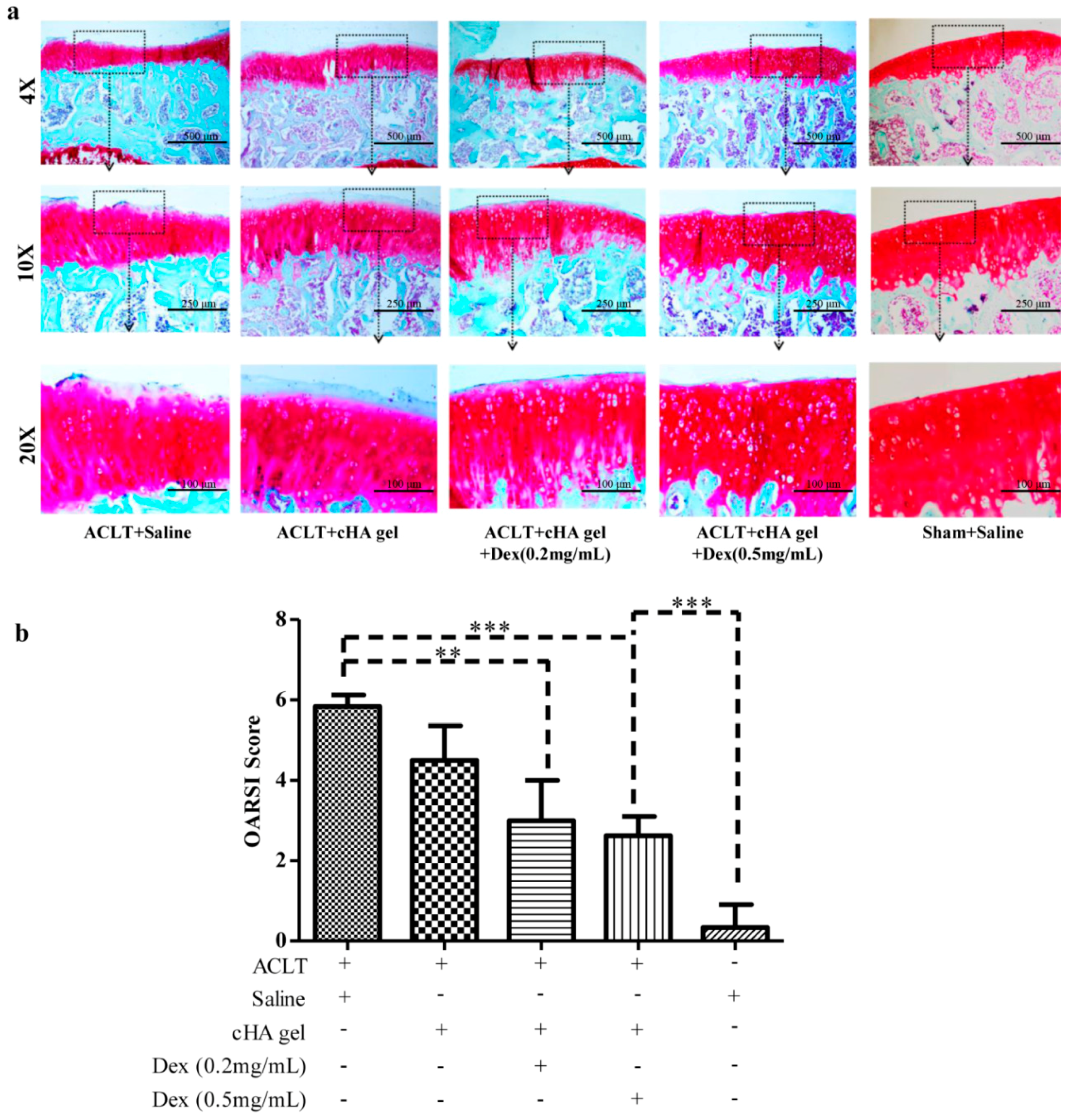
2.3. Intra-Articular cHA-Dex Hydrogel Injections Increased the Expression of Proteoglycan in the Microscopic Appearance of OA Pathology
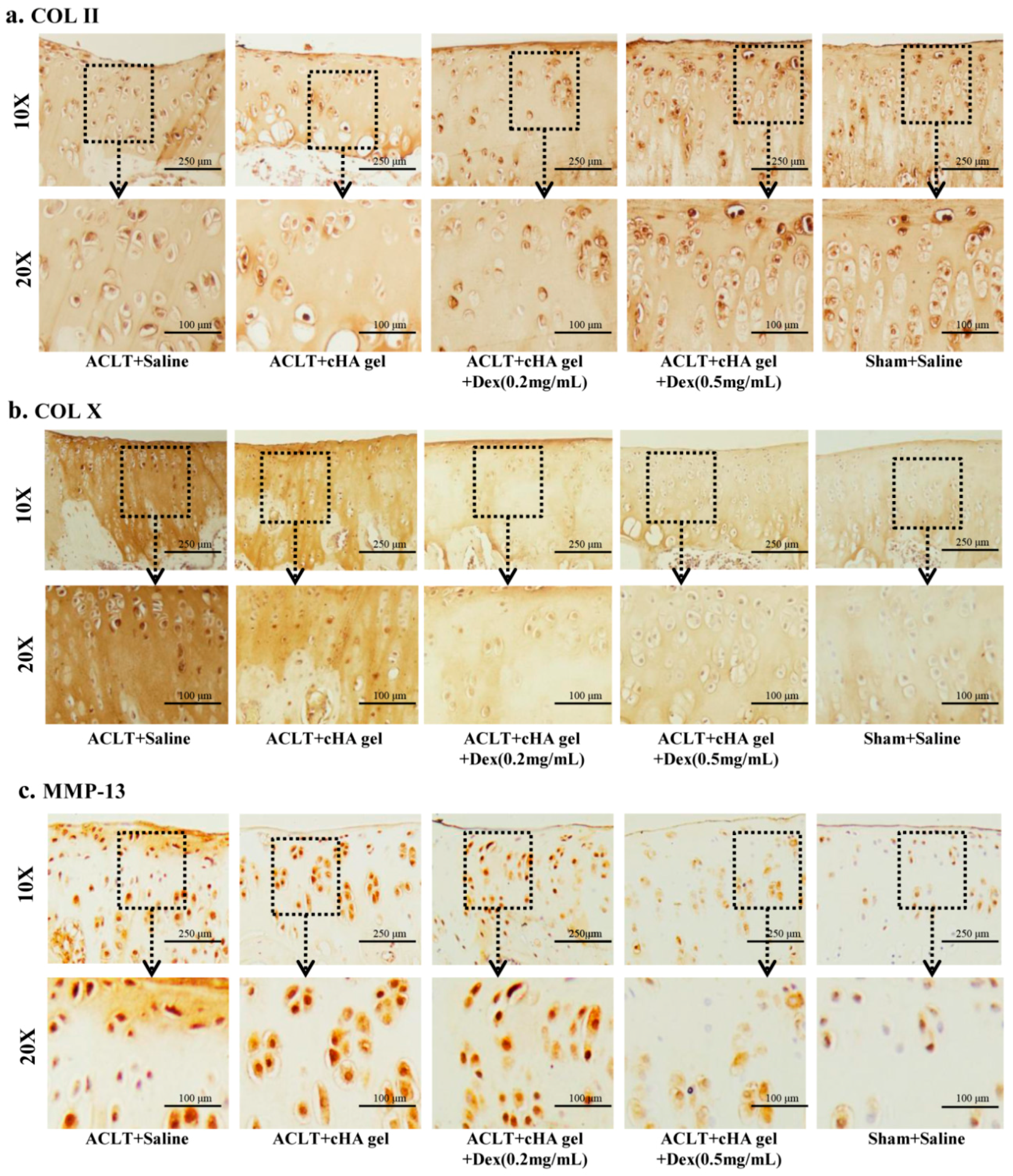
2.4. Intra-Articular cHA-Dex Hydrogel Injections Increased COL II Expression, but Decreased COL X and MMP-13 Expression in Cartilage, Histologically
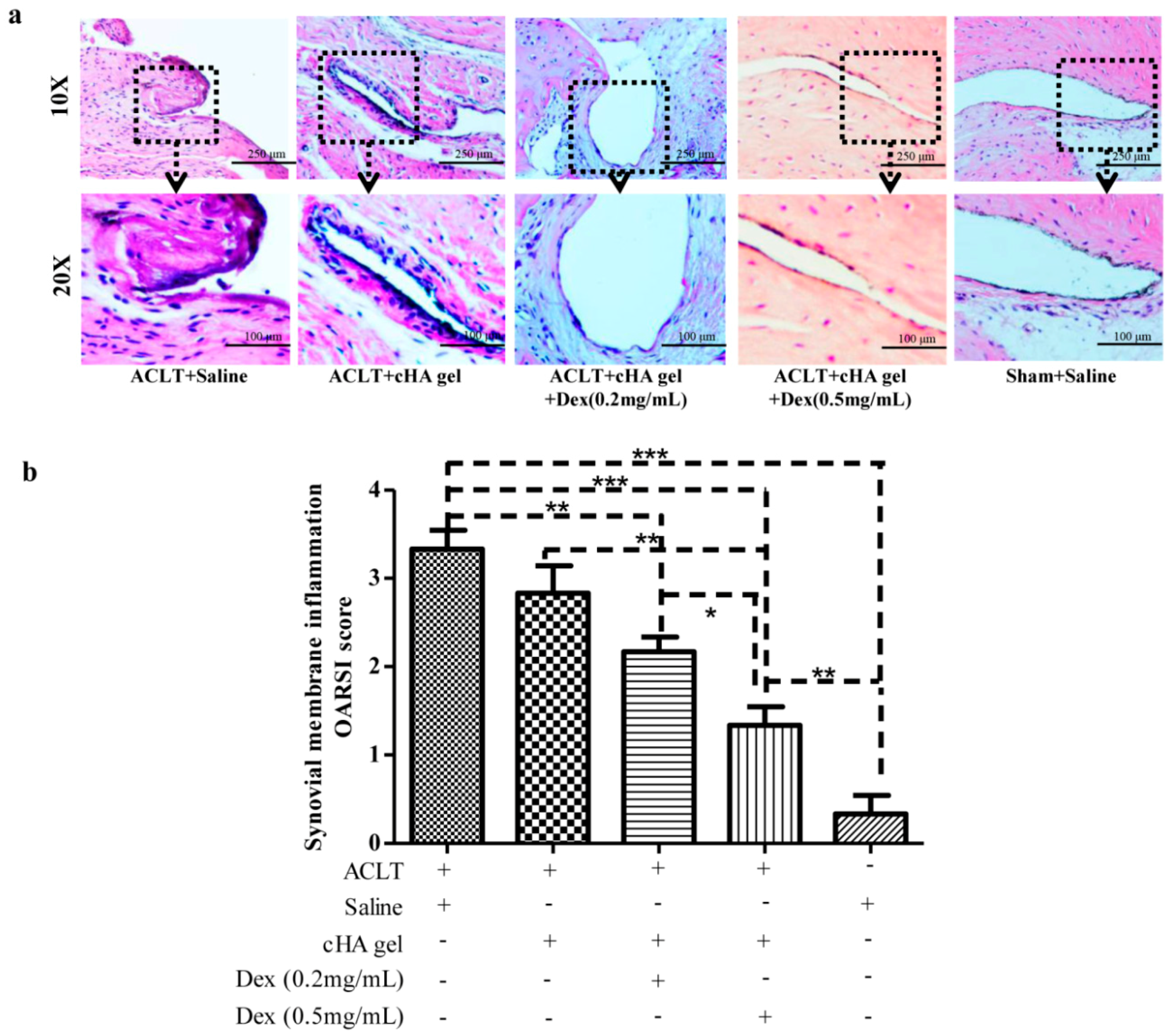
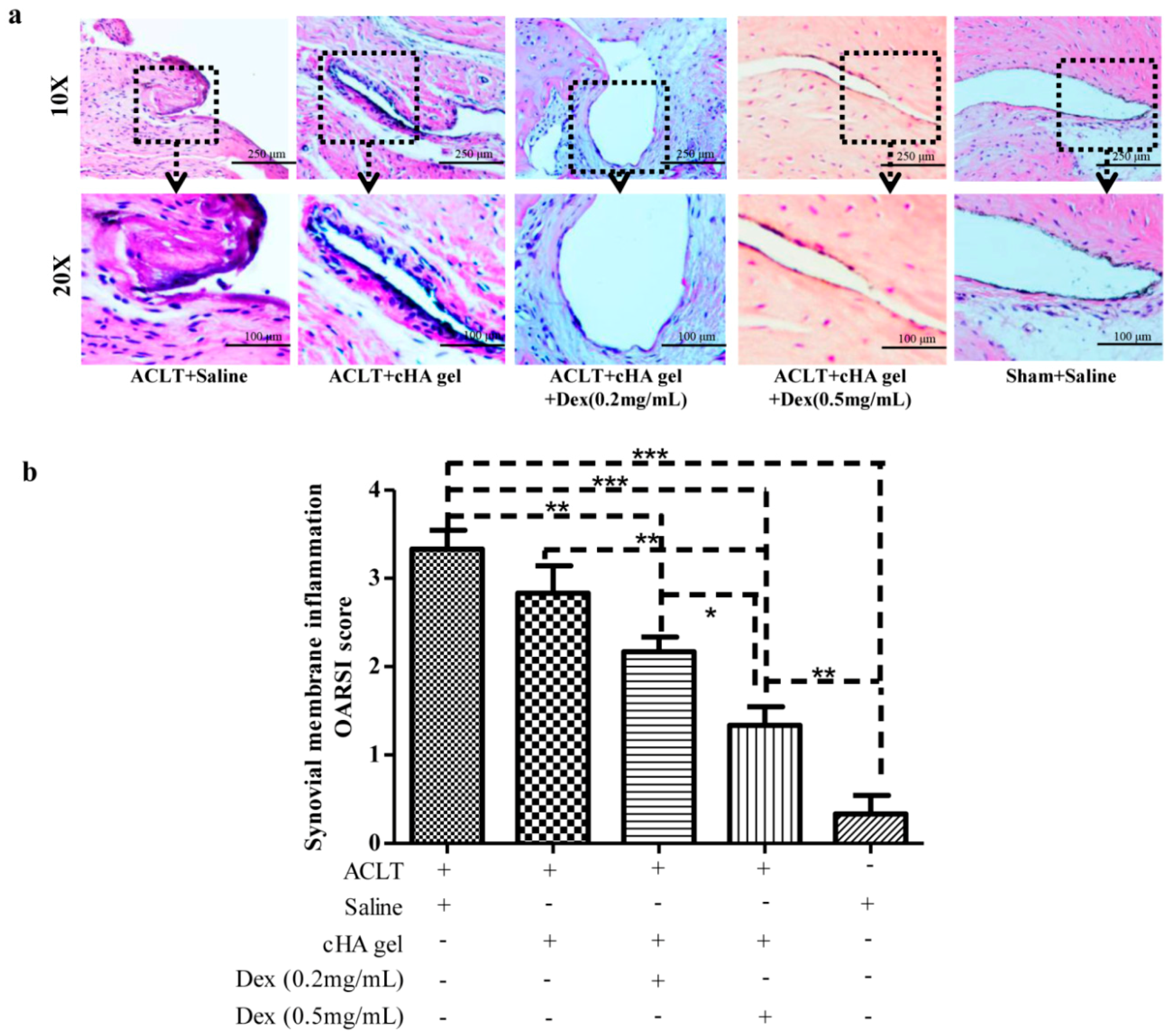
2.5. Intra-Articular cHA-Dex Hydrogel Injections Relieved Synovial Inflammation
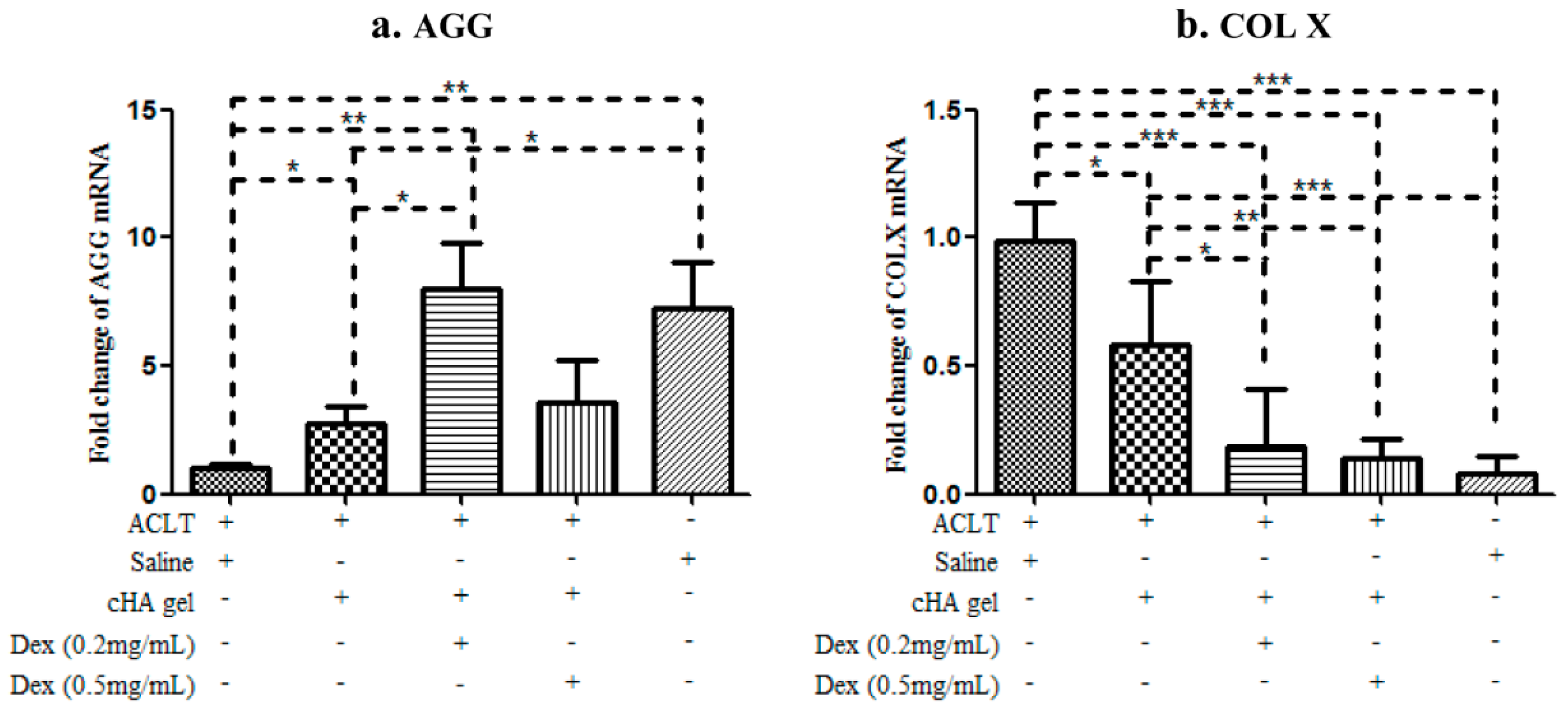
2.6. Intra-Articular cHA-Dex Hydrogel Injections Increased Gene Expression of Aggrecan, but Decreased Type X Collagen
3. Discussion
4. Materials and Methods
4.1. Cell Viability and Toxicity
4.2. Rat Anterior Cruciate Ligament Transection (ACLT) OA Model and Treatment with Intra-Articular cHA-Dex Hydrogel Injections
4.3. Radiography
4.4. Histology
4.5. Immunohistochemistry
4.6. Evaluation of Synovitis
4.7. Quantitative Reverse Transcription Polymerase Chain Reaction (RT-qPCR)
4.8. Statistical Analysis
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Emery, C.A.; Roos, E.M.; Verhagen, E.; Finch, C.F.; Bennell, K.L.; Story, B.; Spindler, K.; Kemp, J.; Lohmander, L.S. Oarsi clinical trials recommendations: Design and conduct of clinical trials for primary prevention of osteoarthritis by joint injury prevention in sport and recreation. Osteoarthritis Cartilage 2015, 23, 815–825. [Google Scholar] [CrossRef] [PubMed]
- Farzaei, M.H.; Farzaei, F.; Gooshe, M.; Abbasabadi, Z.; Rezaei, N.; Abdolghaffari, A.H. Potentially effective natural drugs in treatment for the most common rheumatic disorder: Osteoarthritis. Rheumatol. Int. 2015, 35, 799–814. [Google Scholar] [CrossRef] [PubMed]
- Iannitti, T.; Lodi, D.; Palmieri, B. Intra-articular injections for the treatment of osteoarthritis: Focus on the clinical use of hyaluronic acid. Drugs R D 2011, 11, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Verbruggen, G. Chondroprotective drugs in degenerative joint diseases. Rheumatology 2006, 45, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, J.P.; Martel-Pelletier, J.; Raynauld, J.P. Most recent developments in strategies to reduce the progression of structural changes in osteoarthritis: Today and tomorrow. Arthritis Res. Ther. 2006, 8, 206. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, J.P. Rationale for the use of structure-modifying drugs and agents in the treatment of osteoarthritis. Osteoarthritis Cartilage 2004, 12, S63–S68. [Google Scholar] [CrossRef] [PubMed]
- Altman, R.D.; Hochberg, M.C.; Moskowitz, R.W.; Schnitzer, T.J. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. American college of rheumatology subcommittee on osteoarthritis guidelines. Arthritis Rheum. 2000, 43, 1905–1915. [Google Scholar]
- Zhang, W.; Moskowitz, R.W.; Nuki, G.; Abramson, S.; Altman, R.D.; Arden, N.; Bierma-Zeinstra, S.; Brandt, K.D.; Croft, P.; Doherty, M.; et al. Oarsi recommendations for the management of hip and knee osteoarthritis, part II: Oarsi evidence-based, expert consensus guidelines. Osteoarthritis Cartilage 2008, 16, 137–162. [Google Scholar] [CrossRef] [PubMed]
- Jordan, K.M.; Arden, N.K.; Doherty, M.; Bannwarth, B.; Bijlsma, J.W.; Dieppe, P.; Gunther, K.; Hauselmann, H.; Herrero-Beaumont, G.; Kaklamanis, P.; et al. Eular recommendations 2003: An evidence based approach to the management of knee osteoarthritis: Report of a task force of the standing committee for international clinical studies including therapeutic trials (ESCISIT). Ann. Rheum. Dis. 2003, 62, 1145–1155. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, N.; Campbell, J.; Robinson, V.; Gee, T.; Bourne, R.; Wells, G. Intraarticular corticosteroid for treatment of osteoarthritis of the knee. Cochrane Database Syst. Rev. 2006, CD005328. [Google Scholar] [CrossRef]
- Huebner, K.D.; Shrive, N.G.; Frank, C.B. Dexamethasone inhibits inflammation and cartilage damage in a new model of post-traumatic osteoarthritis. J. Orthop. Res. 2014, 32, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Eyigor, S.; Hepguler, S.; Sezak, M.; Oztop, F.; Capaci, K. Effects of intra-articular hyaluronic acid and corticosteroid therapies on articular cartilage in experimental severe osteoarthritis. Clin. Exp. Rheumatol. 2006, 24, 724. [Google Scholar] [PubMed]
- Derfoul, A.; Perkins, G.L.; Hall, D.J.; Tuan, R.S. Glucocorticoids promote chondrogenic differentiation of adult human mesenchymal stem cells by enhancing expression of cartilage extracellular matrix genes. Stem Cells 2006, 24, 1487–1495. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Goomer, R.S.; Harwood, F.; Kubo, T.; Hirasawa, Y.; Amiel, D. The effects of hyaluronan on matrix metalloproteinase-3 (MMP-3), interleukin-1β(IL-1β), and tissue inhibitor of metalloproteinase-1 (TIMP-1) gene expression during the development of osteoarthritis. Osteoarthritis Cartilage 1999, 7, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Brzusek, D.; Petron, D. Treating knee osteoarthritis with intra-articular hyaluronans. Curr. Med. Res. Opin. 2008, 24, 3307–3322. [Google Scholar] [CrossRef] [PubMed]
- Arnold, W.; Fullerton, D.S.; Holder, S.; May, C.S. Viscosupplementation: Managed care issues for osteoarthritis of the knee. J. Manag. Care Pharm. 2007, 13, S3–S19. [Google Scholar] [CrossRef] [PubMed]
- Larsen, N.E.; Dursema, H.D.; Pollak, C.T.; Skrabut, E.M. Clearance kinetics of a hylan-based viscosupplement after intra-articular and intravenous administration in animal models. J. Biomed. Mater. Res. B Appl. Biomater. 2012, 100, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.J.; Laurent, U.B.; Fraser, J.R. Turnover of hyaluronan in synovial joints: Elimination of labelled hyaluronan from the knee joint of the rabbit. Exp. Physiol. 1991, 76, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; He, X. Intra-articular hyaluronic acid and corticosteroids in the treatment of knee osteoarthritis: A meta-analysis. Exp. Ther. Med. 2015, 9, 493–500. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.T.; Lin, Y.T.; Chiang, B.L.; Lin, Y.H.; Hou, S.M. High molecular weight hyaluronic acid down-regulates the gene expression of osteoarthritis-associated cytokines and enzymes in fibroblast-like synoviocytes from patients with early osteoarthritis. Osteoarthritis Cartilage 2006, 14, 1237–1247. [Google Scholar] [CrossRef] [PubMed]
- Gomis, A.; Miralles, A.; Schmidt, R.F.; Belmonte, C. Nociceptive nerve activity in an experimental model of knee joint osteoarthritis of the guinea pig: Effect of intra-articular hyaluronan application. Pain 2007, 130, 126–136. [Google Scholar] [CrossRef] [PubMed]
- Pozo, M.A.; Balazs, E.A.; Belmonte, C. Reduction of sensory responses to passive movements of inflamed knee joints by hylan, a hyaluronan derivative. Exp. Brain Res. 1997, 116, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Balazs, E.A.; Denlinger, J.L. Viscosupplementation: A new concept in the treatment of osteoarthritis. J. Rheumatol. Suppl. 1993, 39, 3–9. [Google Scholar] [PubMed]
- Elliott, A.L.; Kraus, V.B.; Luta, G.; Stabler, T.; Renner, J.B.; Woodard, J.; Dragomir, A.D.; Helmick, C.G.; Hochberg, M.C.; Jordan, J.M. Serum hyaluronan levels and radiographic knee and hip osteoarthritis in african americans and caucasians in the johnston county osteoarthritis project. Arthritis Rheum. 2005, 52, 105–111. [Google Scholar] [CrossRef] [PubMed]
- Pavelka, K.; Forejtova, S.; Olejarova, M.; Gatterova, J.; Senolt, L.; Spacek, P.; Braun, M.; Hulejova, M.; Stovickova, J.; Pavelkova, A. Hyaluronic acid levels may have predictive value for the progression of knee osteoarthritis. Osteoarthritis Cartilage 2004, 12, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Jiang, D.; Wang, Z.; Wu, G.; Miao, L.; Huang, L. Intra-articular delivery of liposomal celecoxib-hyaluronate combination for the treatment of osteoarthritis in rabbit model. Int. J. Pharm. 2013, 441, 285–290. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.T.; Sheu, M.T.; Lin, Y.F.; Lan, J.; Chin, Y.P.; Hsieh, M.S.; Cheng, C.W.; Chen, C.H. Injectable hyaluronic-acid-doxycycline hydrogel therapy in experimental rabbit osteoarthritis. BMC Vet. Res. 2013, 9, 68. [Google Scholar] [CrossRef] [PubMed]
- Dahl, L.B.; Dahl, I.M.; Engstrom-Laurent, A.; Granath, K. Concentration and molecular weight of sodium hyaluronate in synovial fluid from patients with rheumatoid arthritis and other arthropathies. Ann. Rheum. Dis. 1985, 44, 817–822. [Google Scholar] [CrossRef] [PubMed]
- Elmorsy, S.; Funakoshi, T.; Sasazawa, F.; Todoh, M.; Tadano, S.; Iwasaki, N. Chondroprotective effects of high-molecular-weight cross-linked hyaluronic acid in a rabbit knee osteoarthritis model. Osteoarthritis Cartilage 2014, 22, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Raitcheva, D.; Hawes, M.; Moran, N.; Yu, X.; Wang, F.; Matthews, G.L. Hylan G-F 20 maintains cartilage integrity and decreases osteophyte formation in osteoarthritis through both anabolic and anti-catabolic mechanisms. Osteoarthritis Cartilage 2012, 20, 1336–1346. [Google Scholar] [CrossRef] [PubMed]
- Cao, K.; Wei, L.; Zhang, Z.; Guo, L.; Zhang, C.; Li, Y.; Sun, C.; Sun, X.; Wang, S.; Li, P.; et al. Decreased histone deacetylase 4 is associated with human osteoarthritis cartilage degeneration by releasing histone deacetylase 4 inhibition of runt-related transcription factor-2 and increasing osteoarthritis-related genes: A novel mechanism of human osteoarthritis cartilage degeneration. Arthritis Res. Ther. 2014, 16, 491. [Google Scholar] [CrossRef] [PubMed]
- Jay, G.D.; Fleming, B.C.; Watkins, B.A.; McHugh, K.A.; Anderson, S.C.; Zhang, L.X.; Teeple, E.; Waller, K.A.; Elsaid, K.A. Prevention of cartilage degeneration and restoration of chondroprotection by lubricin tribosupplementation in the rat following anterior cruciate ligament transection. Arthritis Rheum. 2010, 62, 2382–2391. [Google Scholar] [CrossRef] [PubMed]
- Innes, J.F.; Costello, M.; Barr, F.J.; Rudorf, H.; Barr, A.R. Radiographic progression of osteoarthritis of the canine stifle joint: A prospective study. Vet. Radiol. Ultrasound 2004, 45, 143–148. [Google Scholar] [CrossRef] [PubMed]
- Meachim, G. Light microscopy of indian ink preparations of fibrillated cartilage. Ann. Rheum. Dis. 1972, 31, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Gerwin, N.; Bendele, A.M.; Glasson, S.; Carlson, C.S. The oarsi histopathology initiative—Recommendations for histological assessments of osteoarthritis in the rat. Osteoarthritis Cartilage 2010, 18, S24–S34. [Google Scholar] [CrossRef] [PubMed]
- Wei, F.; Zhou, J.; Wei, X.; Zhang, J.; Fleming, B.C.; Terek, R.; Pei, M.; Chen, Q.; Liu, T.; Wei, L. Activation of indian hedgehog promotes chondrocyte hypertrophy and upregulation of MMP-13 in human osteoarthritic cartilage. Osteoarthritis Cartilage 2012, 20, 755–763. [Google Scholar] [CrossRef] [PubMed]



© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Z.; Wei, X.; Gao, J.; Zhao, Y.; Zhao, Y.; Guo, L.; Chen, C.; Duan, Z.; Li, P.; Wei, L. Intra-Articular Injection of Cross-Linked Hyaluronic Acid-Dexamethasone Hydrogel Attenuates Osteoarthritis: An Experimental Study in a Rat Model of Osteoarthritis. Int. J. Mol. Sci. 2016, 17, 411. https://doi.org/10.3390/ijms17040411
Zhang Z, Wei X, Gao J, Zhao Y, Zhao Y, Guo L, Chen C, Duan Z, Li P, Wei L. Intra-Articular Injection of Cross-Linked Hyaluronic Acid-Dexamethasone Hydrogel Attenuates Osteoarthritis: An Experimental Study in a Rat Model of Osteoarthritis. International Journal of Molecular Sciences. 2016; 17(4):411. https://doi.org/10.3390/ijms17040411
Chicago/Turabian StyleZhang, Zhiwei, Xiaochun Wei, Jizong Gao, Yu Zhao, Yamin Zhao, Li Guo, Chongwei Chen, Zhiqing Duan, Pengcui Li, and Lei Wei. 2016. "Intra-Articular Injection of Cross-Linked Hyaluronic Acid-Dexamethasone Hydrogel Attenuates Osteoarthritis: An Experimental Study in a Rat Model of Osteoarthritis" International Journal of Molecular Sciences 17, no. 4: 411. https://doi.org/10.3390/ijms17040411