
Association between Serum Soluble CD154 Levels and Mortality in Patients with Malignant Middle Cerebral Artery Infarction

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Design and Subjects
2.2. Variables Recorded
2.3. Blood Sample Collection
2.4. Laboratory Determinations
2.5. Statistical Methods
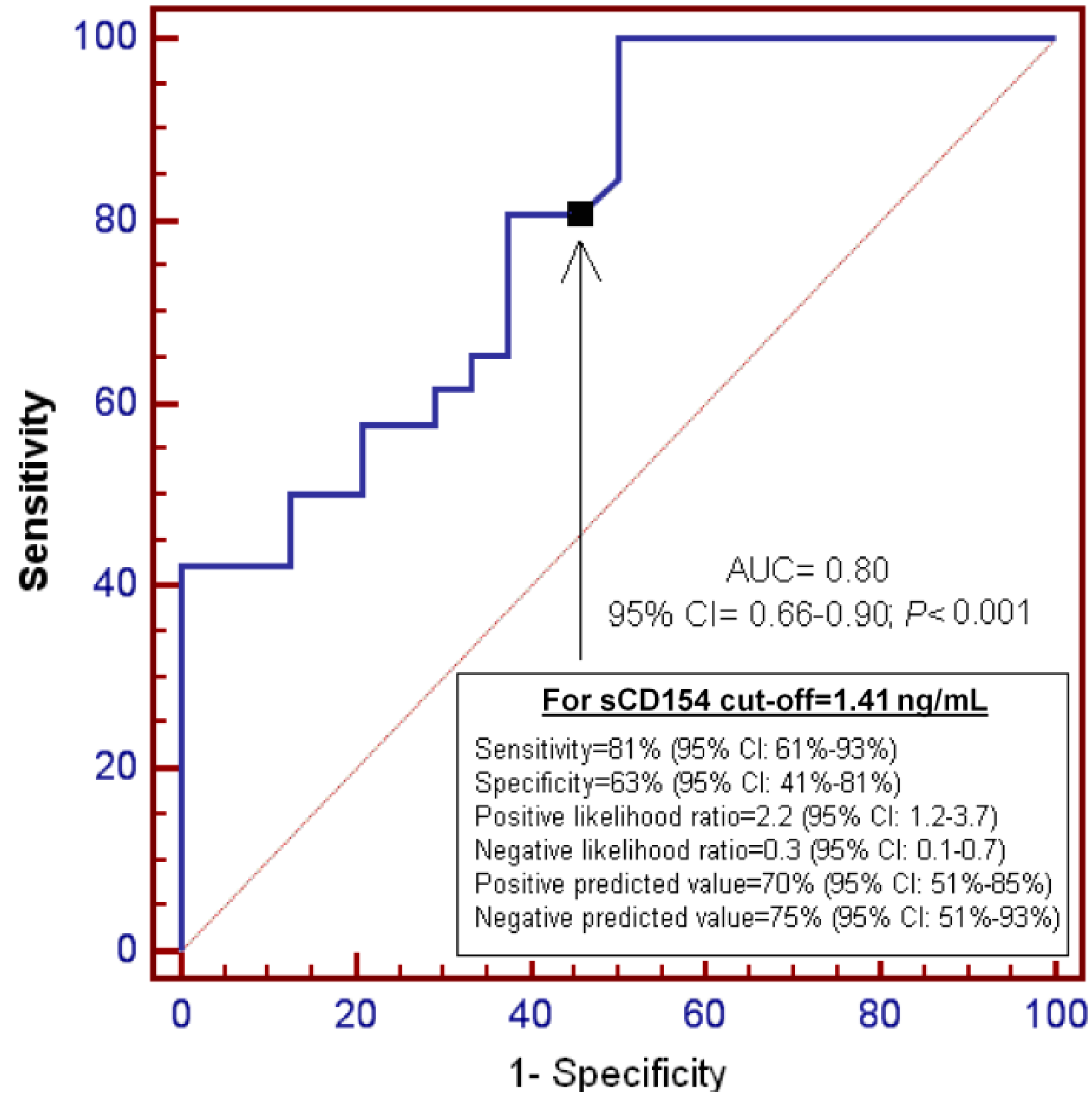
3. Results

{kind=link}
{kind=link}
{kind=link}
| Healthy Controls (n = 50) | Patients (n = 50) | p-Value | |
|---|---|---|---|
| Gender female—n (%) | 15 (30.0%) | 17 (34.0%) | 0.83 |
| Age—median years (p 25–75) | 59 (50–68) | 60 (51–69) | 0.47 |
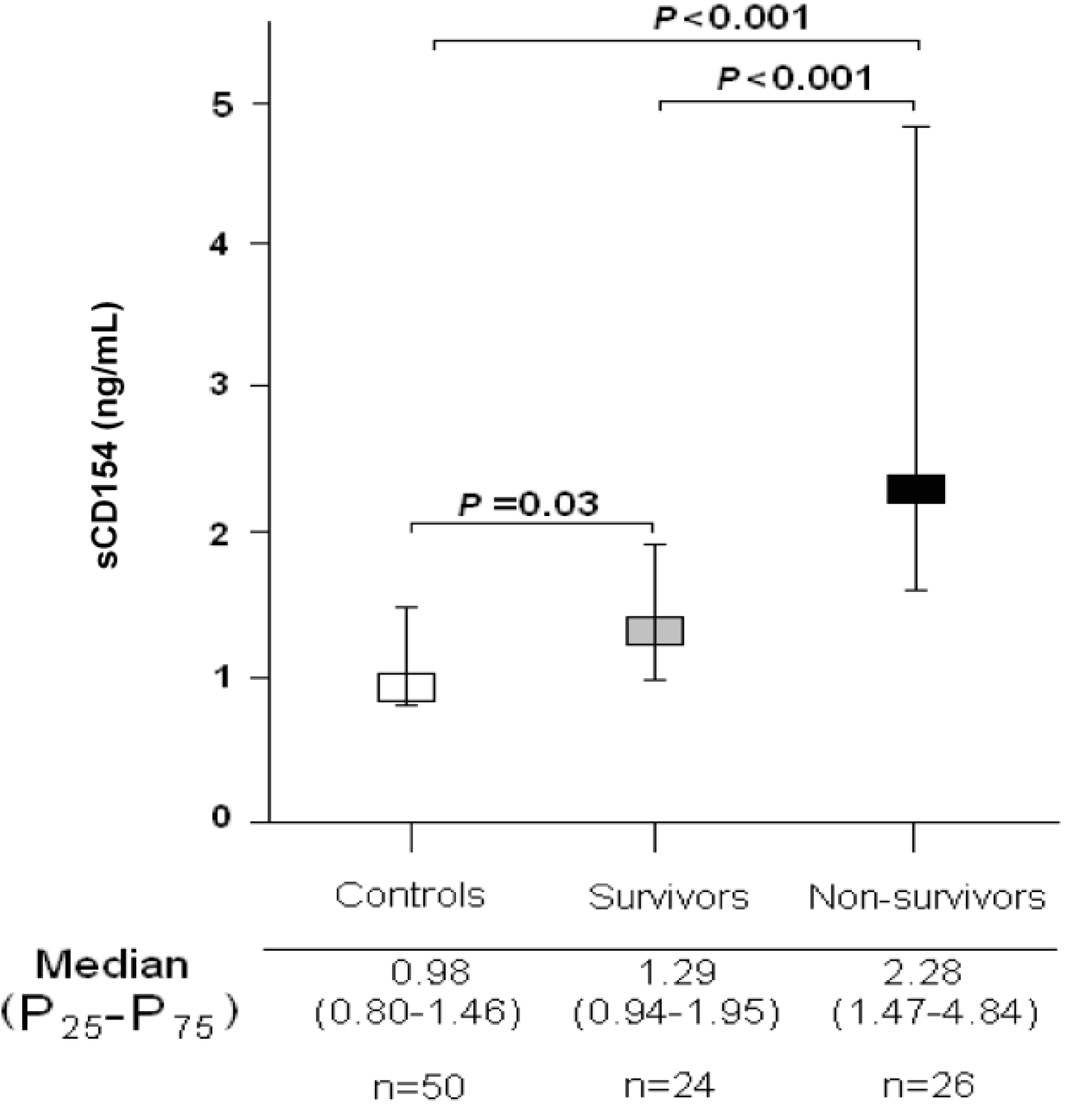
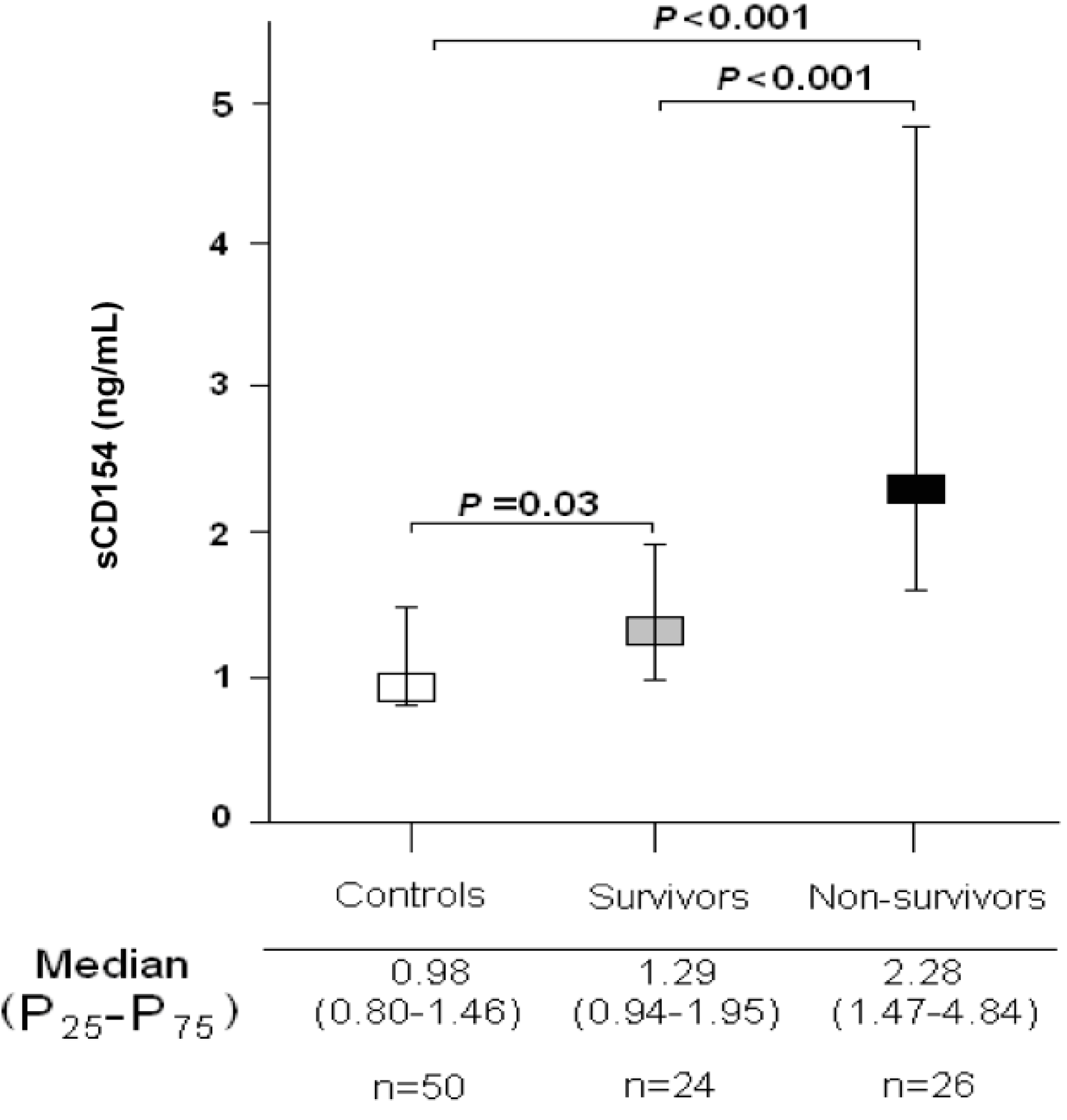
| Serum sCD154—median ng/mL (p 25–75) | 0.98 (0.80–1.46) | 1.79 (1.22–3.56) | <0.001 |
| Survivors (n = 24) | Non-Survivors (n = 26) | p Value | |
|---|---|---|---|
| TNF-alpha (pg/mL)—median (p 25–75) | 9.25 (9.02–10.63) | 12.95 (10.03–15.08) | 0.01 |
| TF (pg/mL)—median (p 25–75) | 156 (127–196) | 279 (181–400) | 0.02 |
| Temperature (°C)—median (p 25–75) | 36.5 (35.7–37.0) | 37.0 (35.7–37.8) | 0.26 |
| Sodium (mEq/L)—median (p 25–75) | 140 (138–145) | 140 (137–146) | 0.91 |
| sCD154 (ng/mL)—median (p 25–75) | 1.29 (0.94–1.95) | 2.28 (1.47–4.84) | <0.001 |
| Platelets—median × 103/mm3 (p 25–75) | 227 (183–308) | 152 (123–190) | 0.003 |
| PaO2 (mmHg)—median (p 25–75) | 110 (101–194) | 104 (85–139) | 0.10 |
| PaO2/FI02 ratio—median (p 25–75) | 246 (192–327) | 248 (175–320) | 0.41 |
| Lymphocytes—median × 103/mm3 (p 25–75) | 1.5 (0.9–1.8) | 1.1 (0.5–2.1) | 0.30 |
| Leukocytes—median × 103/mm3 (p 25–75) | 12.8 (9.8–16.9) | 14.4 (11.9–21.9) | 0.49 |
| Lactic acid (mmol/L)—median (p 25–75) | 1.25 (0.93–1.68) | 1.50 (1.01–3.15) | 0.08 |
| INR—median (p 25–75) | 1.07 (1.01–1.20) | 1.20 (1.07–1.48) | 0.16 |
| Hemoglobin (g/dL)—median (p 25–75) | 12.0 (11.3–13.8) | 12.0 (11.0–15.1) | 0.92 |
| Glycemia (g/dL)—median (p 25–75) | 133 (105–170) | 135 (110–154) | 0.92 |
| GCS score—median (p 25–75) | 7 (6–8) | 6 (4–8) | 0.10 |
| Gender female—n (%) | 8 (33.3) | 9 (34.6) | 0.99 |
| Fibrinogen (mg/dL)—median (p 25–75) | 440 (335–494) | 409 (322–598) | 0.71 |
| Decompressive craniectomy—n (%) | 7 (29.2) | 5 (19.2) | 0.51 |
| Creatinine (mg/dL)—median (p 25–75) | 0.80 (0.60–1.10) | 1.01 (0.85–1.45) | 0.052 |
| Bilirubin (mg/dL)—median (p 25–75) | 0.50 (0.38–0.90) | 0.53 (0.30–1.20) | 0.76 |
| aPTT (seconds)—median (p 25–75) | 28 (25–29) | 26 (25–33) | 0.96 |
| APACHE-II score—median (p 25–75) | 20 (16–25) | 22 (19–29) | 0.14 |
| Age (years)—median (p 25–75) | 47 (32–67) | 66 (45–76) | 0.14 |
| Variable | Odds Ratio | 95% Confidence Interval | p |
|---|---|---|---|
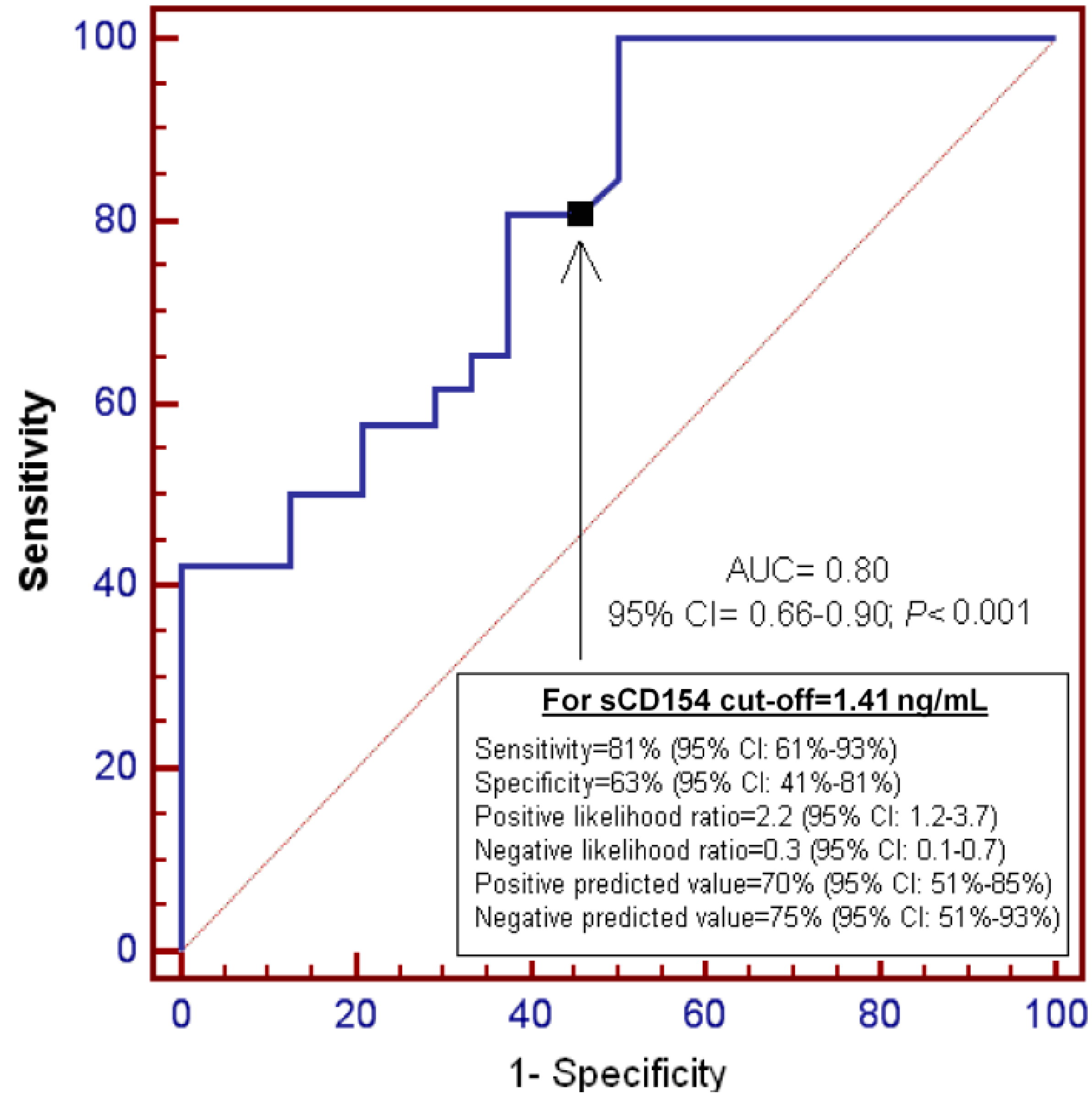
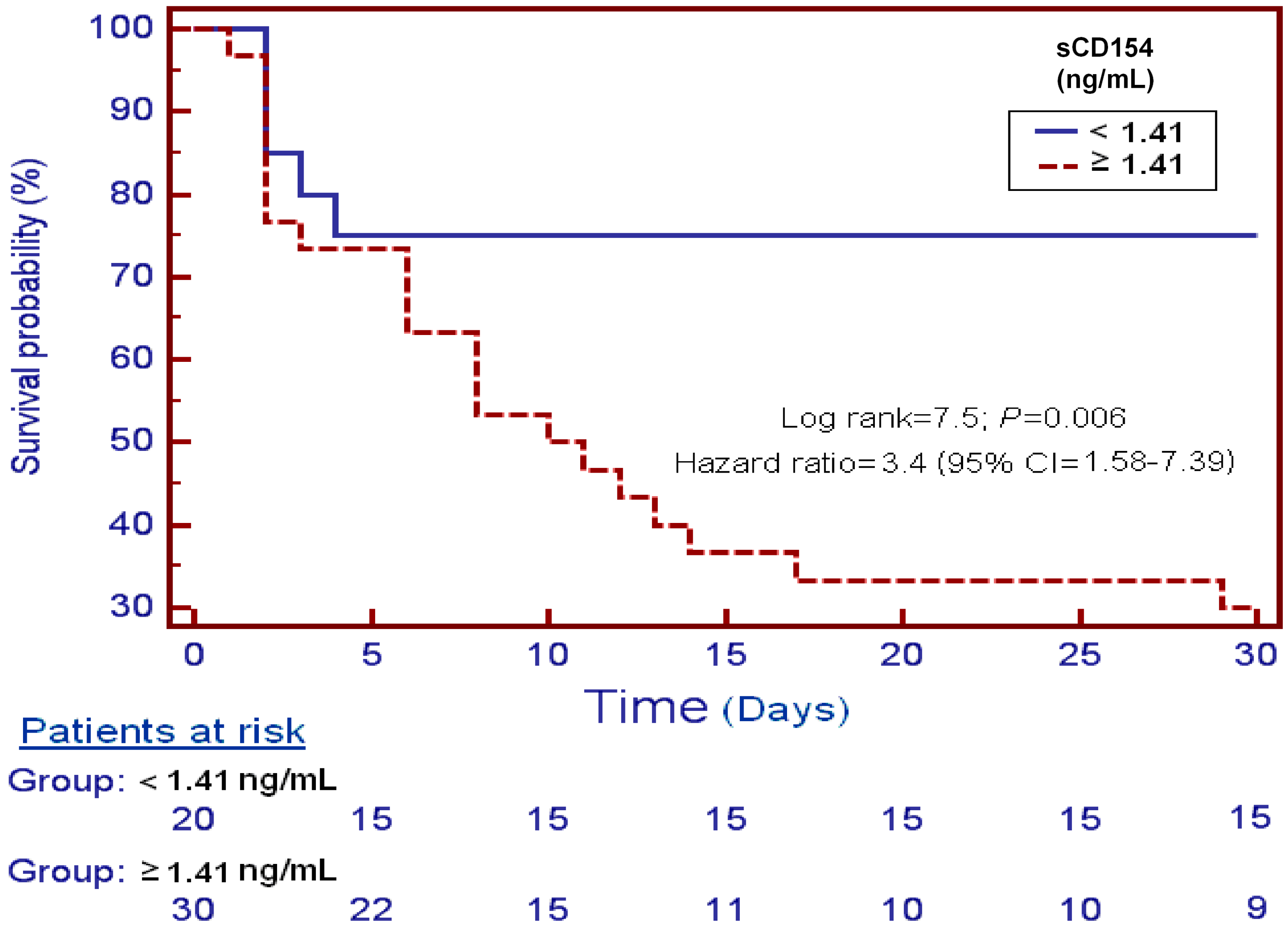
| Serum sCD154 > 1.41 ng/mmL | 10.25 | 2.34–44.95 | 0.002 |
| GCS score | 0.72 | 0.49–1.06 | 0.09 |
| Age (years) | 1.05 | 0.99–1.11 | 0.08 |

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Adams, H.P., Jr.; del Zoppo, G.; Alberts, M.J.; Bhatt, D.L.; Brass, L.; Furlan, A.; Grubb, R.L.; Higashida, R.T.; Jauch, E.C.; Kidwell, C.; et al. Guidelines for the early management of adults with ischemic stroke: A guideline from the American Heart Association/American Stroke Association Stroke Council, Clinical Cardiology Council, Cardiovascular Radiology and Intervention Council, and the Atherosclerotic Peripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary Working Groups: The American Academy of Neurology affirms the value of this guideline as an educational tool for neurologists. Stroke 2007, 38, 1655–1711. [Google Scholar] [PubMed]
- Waid, D.M.; Schreiner, T.; Vaitaitis, G.; Carter, J.R.; Corboy, J.R.; Wagner, D.H., Jr. Defining a new biomarker for the autoimmune component of Multiple Sclerosis: Th40 cells. J. Neuroimmunol. 2014, 270, 75–85. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Wu, T.; Chen, M.; Zhou, Y.; Yi, D.; Guo, R. The CD40/CD40L system: A new therapeutic target for disease. Immunol. Lett. 2013, 153, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Oberheiden, T.; Nguyen, X.D.; Fatar, M.; Elmas, E.; Blahak, C.; Morper, N.; Dempfle, C.E.; Hennerici, M.; Borggrefe, M.; Kälsch, T. Platelet and monocyte activation in acute ischemic stroke—Is there a correlation with stroke etiology? Clin. Appl. Thromb. Hemost. 2012, 18, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.K.; Jeong, M.H.; Jang, J.Y.; Bae, H.R.; Lim, Y.J.; Kim, J.S.; Kim, S.H.; Kim, J.W. Serial measurement of surface expressions of CD63, P-selectin and CD40 ligand on platelets in atherosclerotic ischemic stroke. A possible role of CD40 ligand on platelets in atherosclerotic ischemic stroke. Cerebrovasc. Dis. 2003, 16, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.H.; Zhang, Y.W.; Zhang, P.; Deng, B.Q.; Ding, S.; Wang, Z.K.; Wu, T.; Wang, J. CD40 ligand as a potential biomarker for atherosclerotic instability. Neurol. Res. 2013, 35, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Mao, D.J.; Guo, R.Y.; Tang, Y.C.; Zang, Y.H. Expression of sCD40L in peripheral blood and NF-κBp65 in PBMC of patients with acute progressive cerebral infarction. Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi 2011, 27, 177–179. [Google Scholar] [PubMed]
- Ding, S.; Zhang, M.; Zhao, Y.; Chen, W.; Yao, G.; Zhang, C.; Zhang, P.; Zhang, Y. The role of carotid plaque vulnerability and inflammation in the pathogenesis of acute ischemic stroke. Am. J. Med. Sci. 2008, 336, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Tuttolomondo, A.; di Raimondo, D.; di Sciacca, R.; Casuccio, A.; Bivona, G.; Bellia, C.; Barreca, L.; Serio, A.; D’Aguanno, G.; Ciaccio, M.; et al. Fetuin-A and CD40 L plasma levels in acute ischemic stroke: Differences in relation to TOAST subtype and correlation with clinical and laboratory variables. Atherosclerosis 2010, 208, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Chen, M.; Yang, H.; Wu, T.; Song, C.; Guo, R. Evidence for involvement of the CD40/CD40L system in post-stroke epilepsy. Neurosci. Lett. 2014, 567, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Lukasik, M.; Dworacki, G.; Michalak, S.; Kufel-Grabowska, J.; Watala, C.; Kozubski, W. Chronic hyper-reactivity of platelets resulting in enhanced monocyte recruitment in patients after ischaemic stroke. Platelets 2012, 23, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Novo, S.; Basili, S.; Tantillo, R.; Falco, A.; Davì, V.; Novo, G.; Corrado, E.; Davì, G. Soluble CD40L and cardiovascular risk in asymptomatic low-grade carotid stenosis. Stroke 2005, 36, 673–675. [Google Scholar] [CrossRef] [PubMed]
- Davì, G.; Tuttolomondo, A.; Santilli, F.; Basili, S.; Ferrante, E.; di Raimondo, D.; Pinto, A.; Licata, G. CD40 ligand and MCP-1 as predictors of cardiovascular events in diabetic patients with stroke. J. Atheroscler. Thromb. 2009, 16, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Tsai, N.W.; Chang, W.N.; Shaw, C.F.; Jan, C.R.; Chang, H.W.; Huang, C.R.; Chen, S.D.; Chuang, Y.C.; Lee, L.H.; Wang, H.C.; et al. Levels and value of platelet activation markers in different subtypes of acute non-cardio-embolic ischemic stroke. Thromb. Res. 2009, 124, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Lukasik, M.; Dworacki, G.; Kufel-Grabowska, J.; Watala, C.; Kozubski, W. Upregulation of CD40 ligand and enhanced monocyte-platelet aggregate formation are associated with worse clinical outcome after ischaemic stroke. Thromb. Haemost. 2012, 107, 346–355, (See comment in PubMed Commons below). [Google Scholar] [CrossRef] [PubMed]
- Teasdale, G.; Jennett, B. Assessement of coma and impaired consciousness: A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Varo, N.; de Lemos, J.A.; Libby, P.; Morrow, D.A.; Murphy, S.A.; Nuzzo, R.; Gibson, C.M.; Cannon, C.P.; Braunwald, E.; Schonbeck, U. Soluble CD40L: Risk prediction after acute coronary syndromes. Circulation 2003, 108, 1049–1052. [Google Scholar] [CrossRef] [PubMed]
- Lorente, L.; Martín, M.M.; Varo, N.; Borreguero-León, J.M.; Solé-Violán, J.; Blanquer, J.; Labarta, L.; Díaz, C.; Jiménez, A.; Pastor, E.; et al. Association between serum soluble CD40 ligand levels and mortality in patients with severe sepsis. Crit. Care 2011, 15, R97. [Google Scholar] [CrossRef] [PubMed]
- Martínez de Lizarrondo, S.; Roncal, C.; Calvayrac, O.; Rodríguez, C.; Varo, N.; Purroy, A.; Lorente, L.; Rodríguez, J.A.; Doeuvre, L.; Hervás-Stubbs, S.; et al. Synergistic effect of thrombin and CD40 ligand on endothelial matrix metalloproteinase-10 expression and microparticle generation in vitro and in vivo. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 1477–1487. [Google Scholar] [CrossRef]
- Lorente, L.; Martín, M.M.; González-Rivero, A.F.; Ramos, L.; Argueso, M.; Cáceres, J.J.; Solé-Violán, J.; Serrano, N.; Rodríguez, S.T.; Jiménez, A.; et al. Serum soluble CD40 Ligand levels are associated with severity and mortality of brain trauma injury patients. Thromb. Res. 2014, 134, 832–836. [Google Scholar] [CrossRef] [PubMed]
- Noelle, R.J.; Roy, M.; Shepherd, D.M.; Stamenkovic, I.; Ledbetter, J.A.; Aruffo, A. A 39-kDa protein on activated helper T cells binds CD40 and transduces the signal for cognate activation of B cells. Proc. Natl. Acad. Sci. USA 1992, 9, 6550–6554. [Google Scholar] [CrossRef]
- Mach, F.; Schönbeck, U.; Sukhova, G.K.; Bourcier, T.; Bonnefoy, J.Y.M.; Pober, J.S.; Libby, P. Functional CD40 ligand is expressed on human vascular endothelial cells, smooth muscle cells, and macrophages: Implications for CD40-CD40 ligand signaling in atherosclerosis. Proc. Natl. Acad. Sci. USA 1997, 94, 1931–1936. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Stordeur, P.; de Lavareille, A.; Thielemans, K.; Capel, P.; Goldman, M.; Pradier, O. CD40 engagement on endothelial cells promotes tissue factor-dependent procoagulant activity. Thromb. Haemost. 1998, 79, 1025–1028. [Google Scholar] [PubMed]
- Hezi-Yamit, A.; Wong, P.W.; Bien-Ly, N.; Komuves, L.G.; Prasad, K.S.; Phillips, D.R.; Sinha, U. Synergistic induction of tissue factor by coagulation factor Xa and TNF: Evidence for involvement of negative regulatory signaling cascades. Proc. Natl. Acad. Sci. USA 2005, 102, 12077–12082. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.L.; Yaron, R.; Yellin, M.J. CD40L-CD40 interactions regulate endothelial cell surface tissue factor and thrombomodulin expression. J. Leukoc. Biol. 1998, 63, 373–379. [Google Scholar] [PubMed]
- Slupsky, J.R.; Kalbas, M.; Willuweit, A.; Henn, V.; Kroczek, R.A.; Müller-Berghaus, G. Activated platelets induce tissue factor expression on human umbilical vein endothelial cells by ligation of CD40. Thromb. Haemost. 1998, 80, 1008–1014. [Google Scholar] [PubMed]
- Prasad, K.S.; Andre, P.; He, M.; Bao, M.; Manganello, J.; Phillips, D.R. Soluble CD40 ligand induces beta3 integrin tyrosine phosphorylation and triggers platelet activation by outside-in signaling. Proc. Natl. Acad. Sci. USA 2003, 100, 12367–12371. [Google Scholar] [CrossRef] [PubMed]
- André, P.; Prasad, K.S.; Denis, C.V.; He, M.; Papalia, J.M.; Hynes, R.O.; Phillips, D.R.; Wagner, D.D. CD40L stabilizes arterial thrombi by a beta3 integrin—Dependent mechanism. Nat. Med. 2002, 8, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Menchén, L.; Marín-Jiménez, I.; Arias-Salgado, E.G.; Fontela, T.; Hernández-Sampelayo, P.; Rodríguez, M.C.; Butta, N.V. Matrix metalloproteinase 9 is involved in Crohn’s disease-associated platelet hyperactivation through the release of soluble CD40 ligand. Gut 2009, 58, 920–992. [Google Scholar] [CrossRef] [PubMed]
- D’Erasmo, E.; Acca, M.; Pisani, D.; Volpe, M.S. Neurological state, infarct size and clinical outcome are related to early platelet count decrease in stroke. Gerontology 1993, 39, 276–279. [Google Scholar] [PubMed]
- Li, J.; Zhao, S.P.; Peng, D.Q.; Xu, Z.M.; Zhou, H.N. Early effect of pravastatin on serum soluble CD40L, matrix metalloproteinase-9, and C-reactive protein in patients with acute myocardial infarction. Clin. Chem. 2004, 50, 1696–1699. [Google Scholar] [CrossRef] [PubMed]
- Hamdan, R.; Hajj, F.; Kadry, Z.; Kassab, R.; Salame, E.; Aboujaoude, S.; Azar, R.; Badaoui, G. Benefit and tolerability of the coadministration of ezetimibe and atorvastatin in acute coronary syndrome patients. J. Med. Liban. 2011, 59, 65–69. [Google Scholar] [PubMed]
- Han, S.H.; Koh, K.K.; Quon, M.J.; Lee, Y.; Shin, E.K. The effects of simvastatin, losartan, and combined therapy on soluble CD40 ligand in hypercholesterolemic, hypertensive patients. Atherosclerosis 2007, 190, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Ní Chróinín, D.; Asplund, K.; Åsberg, S.; Callaly, E.; Cuadrado-Godia, E.; Díez-Tejedor, E.; di Napoli, M.; Engelter, S.T.; Furie, K.L.; Giannopoulos, S.; et al. Statin therapy and outcome after ischemic stroke: Systematic review and meta-analysis of observational studies and randomized trials. Stroke 2013, 44, 448–456. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorente, L.; Martín, M.M.; González-Rivero, A.F.; Ramos, L.; Argueso, M.; Cáceres, J.J.; Solé-Violán, J.; Jiménez, A.; Borreguero-León, J.M. Association between Serum Soluble CD154 Levels and Mortality in Patients with Malignant Middle Cerebral Artery Infarction. Int. J. Mol. Sci. 2015, 16, 12147-12158. https://doi.org/10.3390/ijms160612147
Lorente L, Martín MM, González-Rivero AF, Ramos L, Argueso M, Cáceres JJ, Solé-Violán J, Jiménez A, Borreguero-León JM. Association between Serum Soluble CD154 Levels and Mortality in Patients with Malignant Middle Cerebral Artery Infarction. International Journal of Molecular Sciences. 2015; 16(6):12147-12158. https://doi.org/10.3390/ijms160612147
Chicago/Turabian StyleLorente, Leonardo, María M. Martín, Agustín F. González-Rivero, Luis Ramos, Mónica Argueso, Juan J. Cáceres, Jordi Solé-Violán, Alejandro Jiménez, and Juan M. Borreguero-León. 2015. "Association between Serum Soluble CD154 Levels and Mortality in Patients with Malignant Middle Cerebral Artery Infarction" International Journal of Molecular Sciences 16, no. 6: 12147-12158. https://doi.org/10.3390/ijms160612147