
The Effect of Interferon-γ and Zoledronate Treatment on Alpha-Tricalcium Phosphate/Collagen Sponge-Mediated Bone-Tissue Engineering

 , ,
, ,
Abstract
:
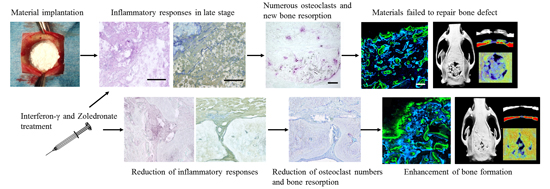
1. Introduction
2. Results
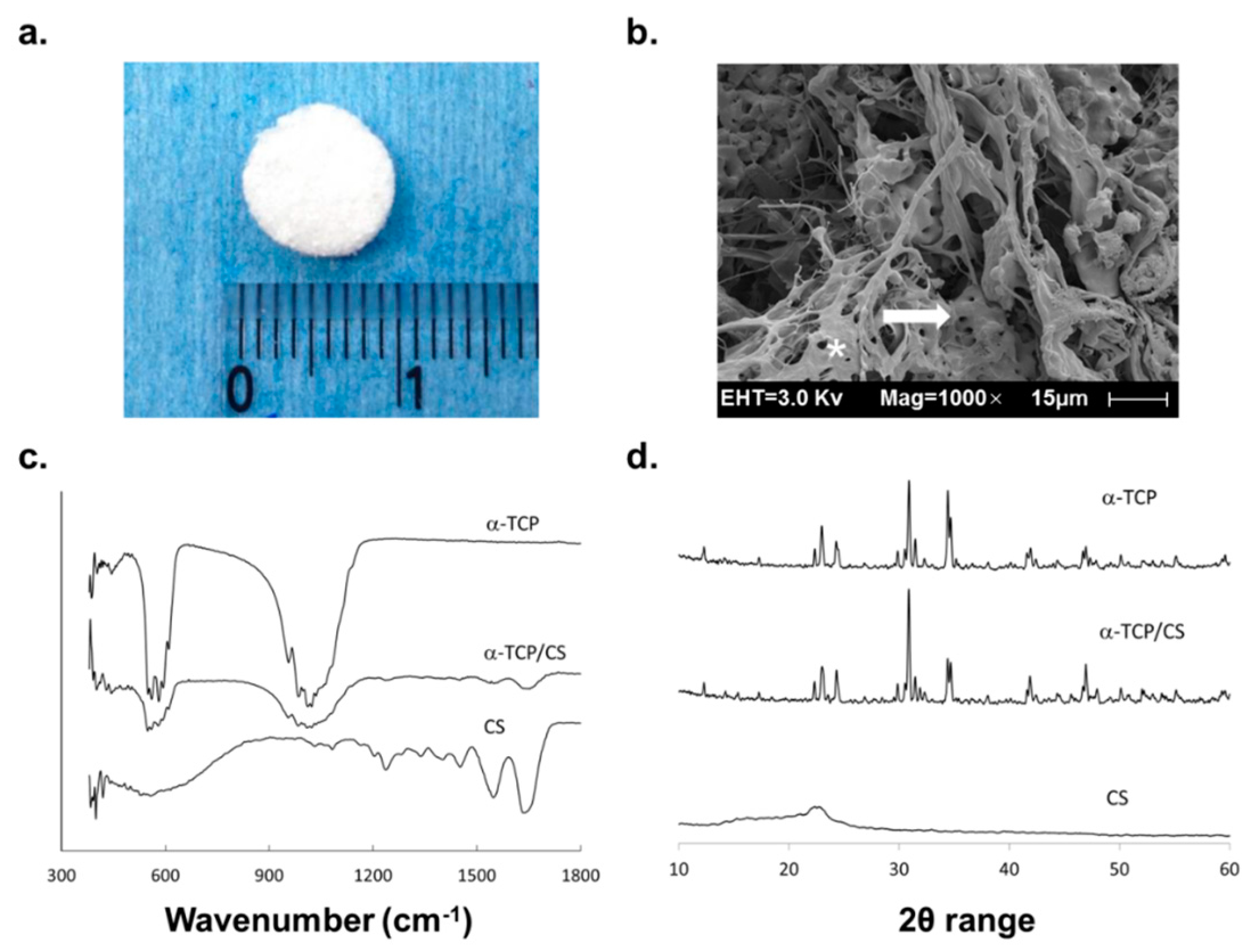
2.1. Material Observations and Measurements
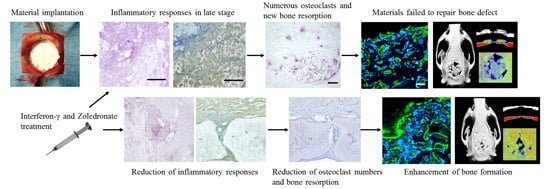
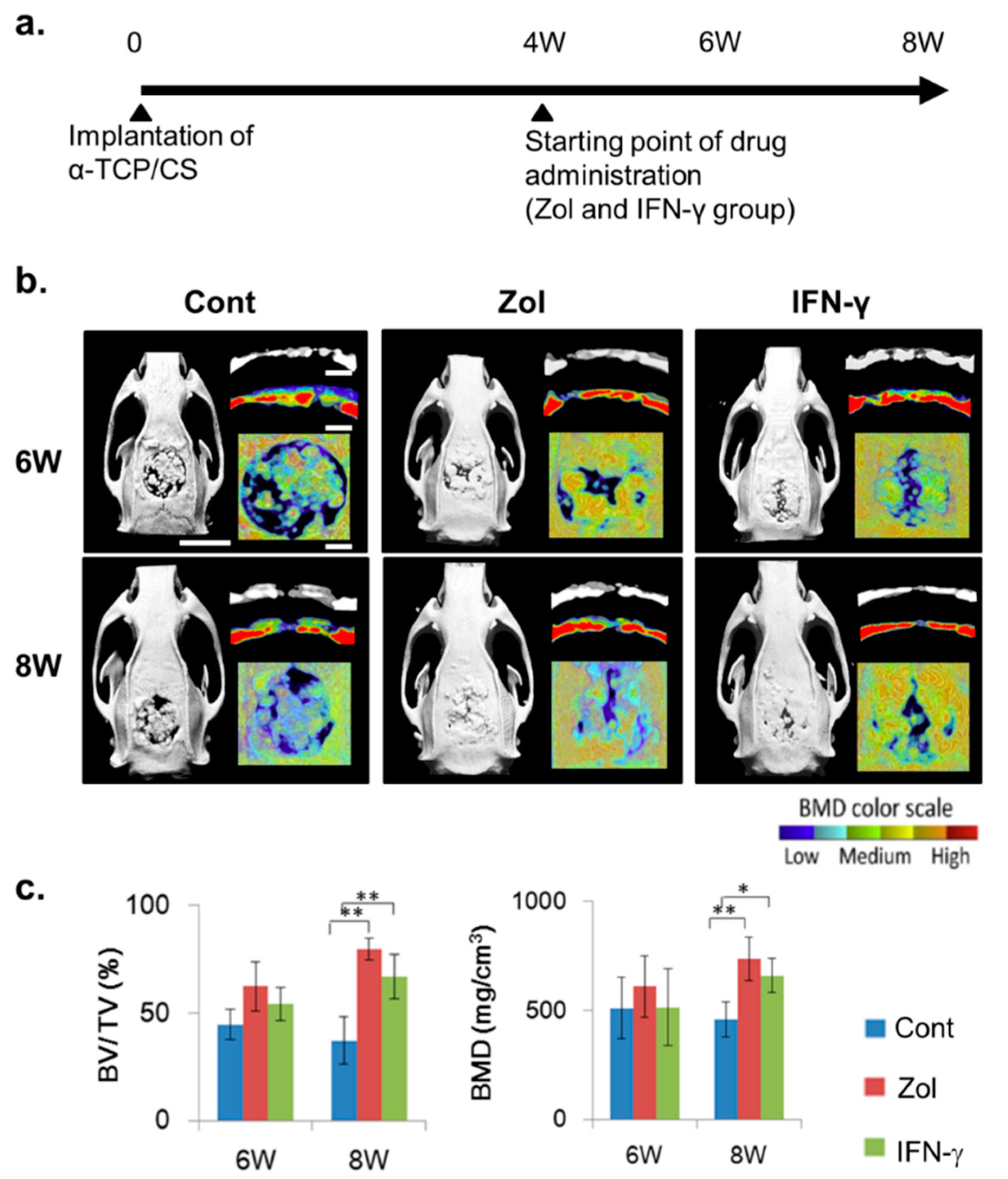
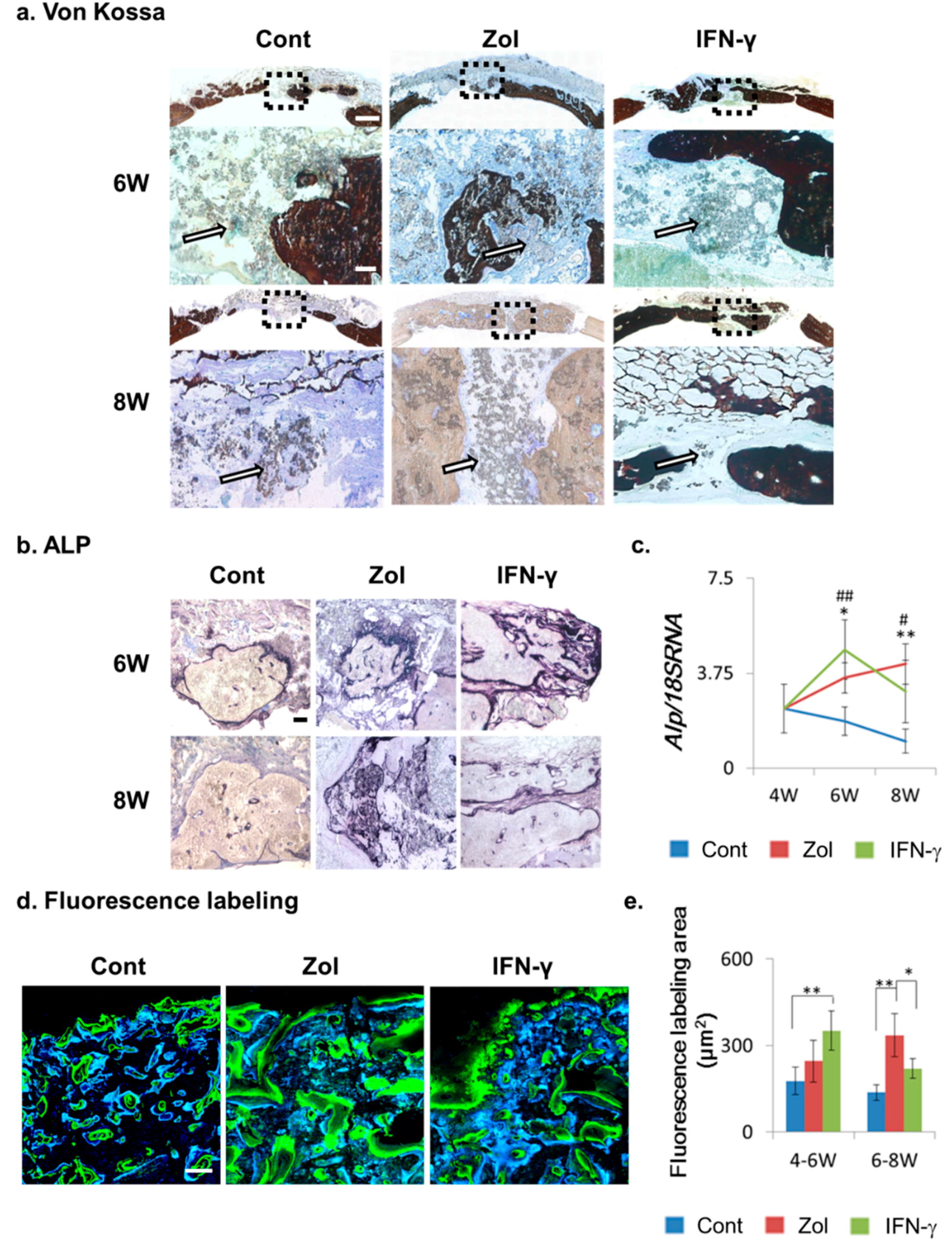
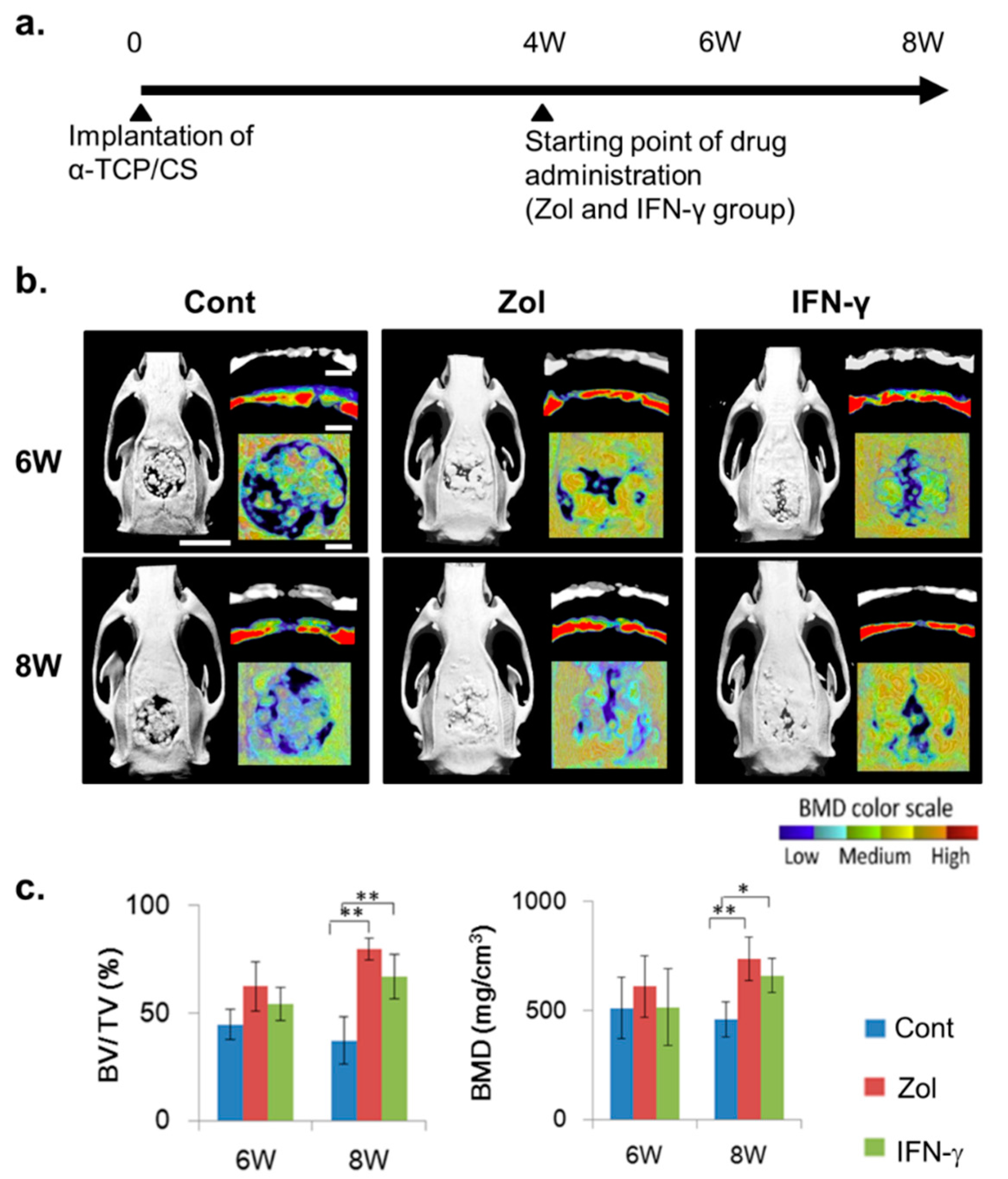
2.2. Effect of Local IFN-γ and Zol Administration on Bone Turnover after Material Implantation
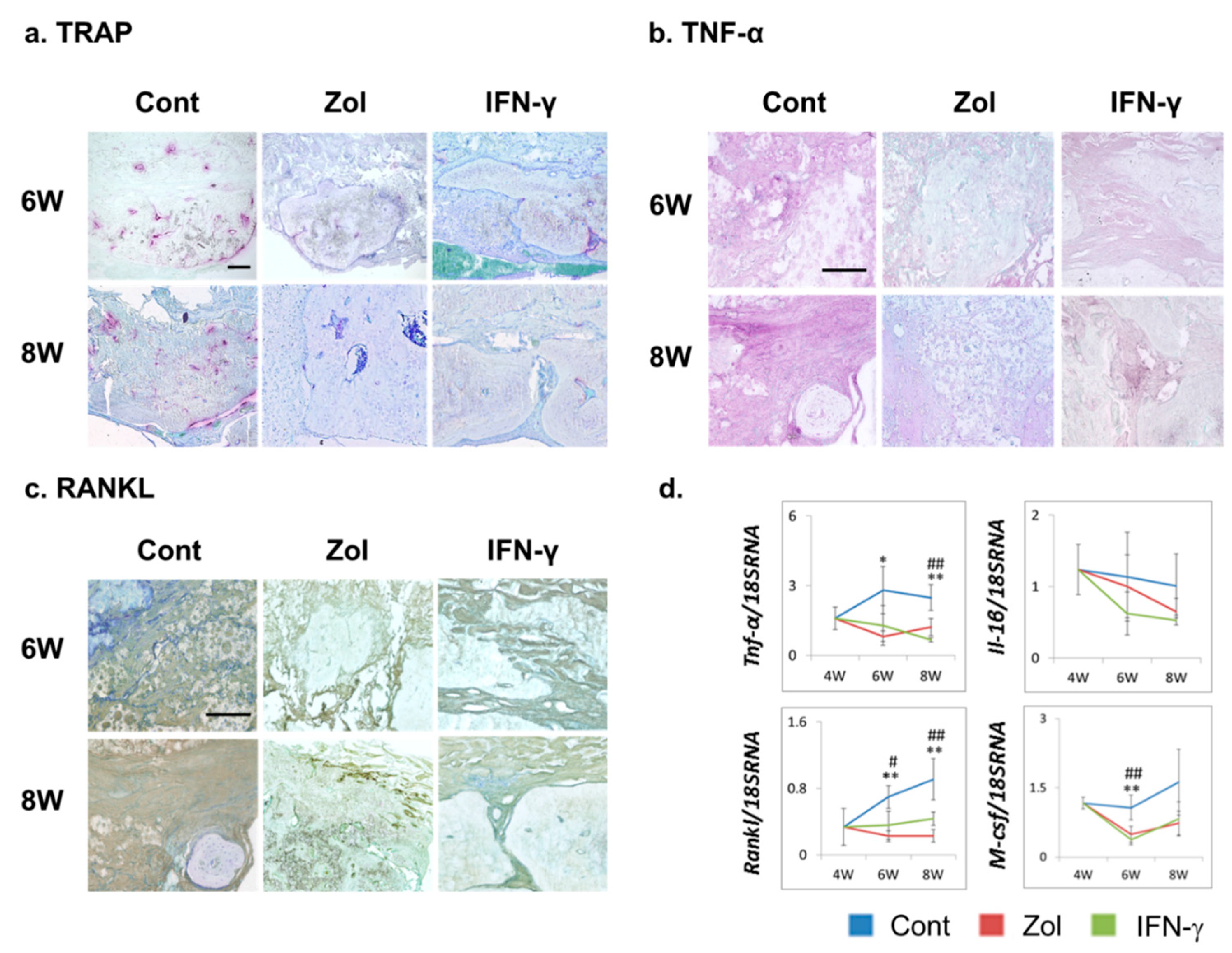
2.3. Effect of Local IFN-γ and Zol Administration on Osteoclastogenesis and TNF-α and RANKL Expression

3. Discussion
4. Experimental Section
4.1. Biomaterial Preparation
4.2. Biomaterial Measurements
4.3. Rat Calvarial-Defect Model
4.4. Evaluation of Osteogenesis in Vivo
4.4.1. Micro-CT and Analysis
4.4.2. RT-PCR and Immunostaining Experiments

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Sequence | #Probe | Accession | |
|---|---|---|---|---|
| Rankl | Forward | 5ʹ-AGACACAGAAGCACTACCTGACTC-3ʹ | #2 | NM_057149 |
| Reverse | 5ʹ-GGCCCACAATGTGTTGTA-3ʹ | |||
| M-csf | Forward | 5ʹ-CAAGGACTATAAGGAACAGAACGAG-3ʹ | #55 | NM_023981.4 |
| Reverse | 5ʹ-GAAATTCTTGATTTTCTCCAGCA-3ʹ | |||
| Tnf-α | Forward | 5ʹ-GCCCAGACCCTCACACTC-3ʹ | #119 | X66539.1 |
| Reverse | 5ʹ-CCACTCCAGCTGCTCCTC-3ʹ | |||
| Il-1β | Forward | 5ʹ-TGTGATGAAAGACGGCACAC-3ʹ | #78 | NM_031512.2 |
| Reverse | 5ʹ-CTTCTTCTTTGGGTATTGTTTGG-3ʹ | |||
| Alp | Forward | 5ʹ-GCACAACATCAAGGACATCG-3ʹ | #77 | NM_013059.1 |
| Reverse | 5ʹ-TCAGTTCTGTTCTTGGGGTACAT-3ʹ | |||
4.4.3. Bone Histomorphometry
4.4.4. Histochemical Staining and Histological Observations
4.5. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lee, S.W.; Hahn, B.D.; Kang, T.Y.; Lee, M.J.; Choi, J.Y.; Kim, M.K.; Kim, S.G. Hydroxyapatite and collagen combination-coated dental implants display better bone formation in the peri-implant area than the same combination plus bone morphogenetic protein-2-coated implants, hydroxyapatite only coated implants, and uncoated implants. J. Oral Maxillofac. Surg. 2014, 72, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Arima, Y.; Uemura, N.; Hashimoto, Y.; Baba, S.; Matsumoto, N. Evaluation of bone regeneration by porous alpha-tricalcium phosphate/atelocollagen sponge composite in rat calvarial defects. Orthod. Waves 2013, 72, 23–29. [Google Scholar] [CrossRef]
- Franz, S.; Rammelt, S.; Scharnweber, D.; Simon, J.C. Immune responses to implants—A review of the implications for the design of immunomodulatory biomaterials. Biomaterials 2011, 32, 6692–6709. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.M.; Rodriguez, A.; Chang, D.T. Foreign body reaction to biomaterials. Semin. Immunol. 2008, 20, 86–100. [Google Scholar] [CrossRef] [PubMed]
- Lange, T.; Schilling, A.F.; Peters, F.; Haag, F.; Morlock, M.M.; Rueger, J.M.; Amling, M. Proinflammatory and osteoclastogenic effects of beta-tricalciumphosphate and hydroxyapatite particles on human mononuclear cells in vitro. Biomaterials 2009, 30, 5312–5318. [Google Scholar] [CrossRef] [PubMed]
- Van der Meulen, J.; Koerten, H.K. Inflammatory response and degradation of three types of calcium phosphate ceramic in a non-osseous environment. J. Biomed. Mater. Res. 1994, 28, 1455–1463. [Google Scholar] [CrossRef] [PubMed]
- Tuan, R.S.; Lee, F.Y.-I.; T Konttinen, Y.; Wilkinson, J.M.; Smith, R.L. What are the local and systemic biologic reactions and mediators to wear debris, and what host factors determine or modulate the biologic response to wear particles? J. Am. Acad. Orthop. Surg. 2008, 16, 42–48. [Google Scholar]
- Schutte, R.J.; Xie, L.; Klitzman, B.; Reichert, W.M. In vivo cytokine-associated responses to biomaterials. Biomaterials. 2009, 30, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Ingham, E.; Fisher, J. The role of macrophages in osteolysis of total joint replacement. Biomaterials 2005, 26, 1271–1286. [Google Scholar] [CrossRef] [PubMed]
- Curran, J.M.; Gallagher, J.A.; Hunt, J.A. The inflammatory potential of biphasic calcium phosphate granules in osteoblast/macrophage co-culture. Biomaterials 2005, 26, 5313–5320. [Google Scholar] [CrossRef] [PubMed]
- Schilling, A.F.; Linhart, W.; Filke, S.; Gebauer, M.; Schinke, T.; Rueger, J.M.; Amling, M. Resorbability of bone substitute biomaterials by human osteoclasts. Biomaterials 2004, 25, 3963–3972. [Google Scholar] [CrossRef] [PubMed]
- Clohisy, J.C.; Frazier, E.; Hirayama, T.; Abu-Amer, Y. RANKL is an essential cytokine mediator of polymethylmethacrylate particle-induced osteoclastogenesis. J. Orthop. Res. 2003, 21, 202–212. [Google Scholar] [CrossRef]
- Pyo, S.W.; Kim, Y.M.; Kim, C.S.; Lee, I.S.; Park, J.U. Bone formation on biomimetic calcium phosphate-coated and zoledronate-immobilized titanium implants in osteoporotic rat tibiae. Int. J. Oral Maxillofac. Implant. 2014, 29, 478–484. [Google Scholar] [CrossRef] [PubMed]
- Mosser, D.M.; Edwards, J.P. Exploring the full spectrum of macrophage activation. Nat. Rev. Immunol. 2008, 8, 958–969. [Google Scholar] [CrossRef] [PubMed]
- Kohara, H.; Kitaura, H.; Fujimura, Y.; Yoshimatsu, M.; Morita, Y.; Eguchi, T.; Masuyama, R.; Yoshida, N. IFN-γ directly inhibits TNF-α-induced osteoclastogenesis in vitro and in vivo and induces apoptosis mediated by Fas/Fas ligand interactions. Immunol. Lett. 2011, 137, 53–61. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.D.; Park-Min, K.H.; Shen, Z.; Fajardo, R.J.; Goldring, S.R.; McHugh, K.P.; Ivashkiv, L.B. Inhibition of RANK expression and osteoclastogenesis by TLRs and IFN-γ in human osteoclast precursors. J. Immunol. 2009, 183, 7223–7233. [Google Scholar] [CrossRef] [PubMed]
- Duque, G.; Huang, D.C.; Dion, N.; MacOritto, M.; Rivas, D.; Li, W.; Yang, X.F.; Li, J.; Lian, J.; Marino, F.T.; et al. Interferon-γ plays a role in bone formation in vivo and rescues osteoporosis in ovariectomized mice. J. Bone Miner. Res. 2011, 26, 1472–1483. [Google Scholar] [CrossRef] [PubMed]
- Duque, G.; Huang, D.C.; Macoritto, M.; Rivas, D.; Yang, X.F.; Ste-Marie, L.G.; Kremer, R. Autocrine regulation of interferon gamma in mesenchymal stem cells plays a role in early osteoblastogenesis. Stem Cell 2009, 27, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Gao, Y.; Grassi, F.; Ryan, M.R.; Terauchi, M.; Page, K.; Yang, X.; Weitzmann, M.N.; Pacifici, R. IFN-γ stimulates osteoclast formation and bone loss in vivo via antigen-driven T cell activation. J. Clin. Investig. 2007, 117, 122–132. [Google Scholar] [CrossRef] [PubMed]
- Kitaura, H.; Kimura, K.; Ishida, M.; Kohara, H.; Yoshimatsu, M.; Takano-Yamamoto, T. Immunological reaction in TNF-α-mediated osteoclast formation and bone resorption in vitro and in vivo. Clin. Dev. Immunol. 2013, 2013, 181849. [Google Scholar] [CrossRef] [PubMed]
- Gandolfi, M.G.; Ciapetti, G.; Taddei, P.; Perut, F.; Tinti, A.; Cardoso, M.V.; van Meerbeek, B.; Prati, C. Apatite formation on bioactive calcium-silicate cements for dentistry affects surface topography and human marrow stromal cells proliferation. Dent. Mater. 2010, 26, 974–992. [Google Scholar] [CrossRef] [PubMed]
- De Campos Vidal, B.; Mello, M.L.S. Collagen type I amide I band infrared spectroscopy. Micron 2011, 42, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Rojbani, H.; Nyan, M.; Ohya, K.; Kasugai, S. Evaluation of the osteoconductivity of α-tricalcium phosphate, β-tricalcium phosphate, and hydroxyapatite combined with or without simvastatin in rat calvarial defect. J. Biomed. Mater. Res. A 2011, 98, 488–498. [Google Scholar] [CrossRef] [PubMed]
- Ingram, J.H.; Stone, M.; Fisher, J.; Ingham, E. The influence of molecular weight, crosslinking and counterface roughness on TNF-alpha production by macrophages in response to ultra high molecular weight polyethylene particles. Biomaterials 2004, 25, 3511–3522. [Google Scholar] [CrossRef] [PubMed]
- Gretzer, C.; Emanuelsson, L.; Liljensten, E.; Thomsen, P. The inflammatory cell influx and cytokines changes during transition from acute inflammation to fibrous repair around implanted materials. J. Biomater. Sci. 2006, 17, 669–687. [Google Scholar] [CrossRef]
- Takayanagi, H.; Sato, K.; Takaoka, A.; Taniguchi, T. Interplay between interferon and other cytokine systems in bone metabolism. Immunol. Rev. 2005, 208, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Hong, Z.F.; Huang, X.J.; Yin, Z.Y.; Zhao, W.X.; Wang, X.M. Immunosuppressive function of bone marrow mesenchymal stem cells on acute rejection of liver allografts in rats. Transplant. Proc. 2009, 41, 403–409. [Google Scholar] [CrossRef] [PubMed]
- Emmez, H.; Kardes, O.; Dogulu, F.; Kurt, G.; Memis, L.; Baykaner, M.K. Role of antifibrotic cytokine interferon-γ in the prevention of postlaminectomy peridural fibrosis in rats. Neurosurgery 2008, 62, 1351–1357. [Google Scholar] [CrossRef] [PubMed]
- Kawamoto, T.; Kawamoto, K. Preparation of thin frozen sections from nonfixed and undecalcified hard tissues using kawamot’s film method (2012). Methods Mol. Biol. 2014, 1130, 149–164. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, P.; Hashimoto, Y.; Honda, Y.; Arima, Y.; Matsumoto, N. The Effect of Interferon-γ and Zoledronate Treatment on Alpha-Tricalcium Phosphate/Collagen Sponge-Mediated Bone-Tissue Engineering. Int. J. Mol. Sci. 2015, 16, 25678-25690. https://doi.org/10.3390/ijms161025678
Li P, Hashimoto Y, Honda Y, Arima Y, Matsumoto N. The Effect of Interferon-γ and Zoledronate Treatment on Alpha-Tricalcium Phosphate/Collagen Sponge-Mediated Bone-Tissue Engineering. International Journal of Molecular Sciences. 2015; 16(10):25678-25690. https://doi.org/10.3390/ijms161025678
Chicago/Turabian StyleLi, Peiqi, Yoshiya Hashimoto, Yoshitomo Honda, Yoshiyuki Arima, and Naoyuki Matsumoto. 2015. "The Effect of Interferon-γ and Zoledronate Treatment on Alpha-Tricalcium Phosphate/Collagen Sponge-Mediated Bone-Tissue Engineering" International Journal of Molecular Sciences 16, no. 10: 25678-25690. https://doi.org/10.3390/ijms161025678