Exploring the Role of Paraoxonases in the Pathogenesis of Coronary Artery Disease: A Systematic Review


Abstract
:1. Introduction
2. Methodology and Search Strategy
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction
3. Results
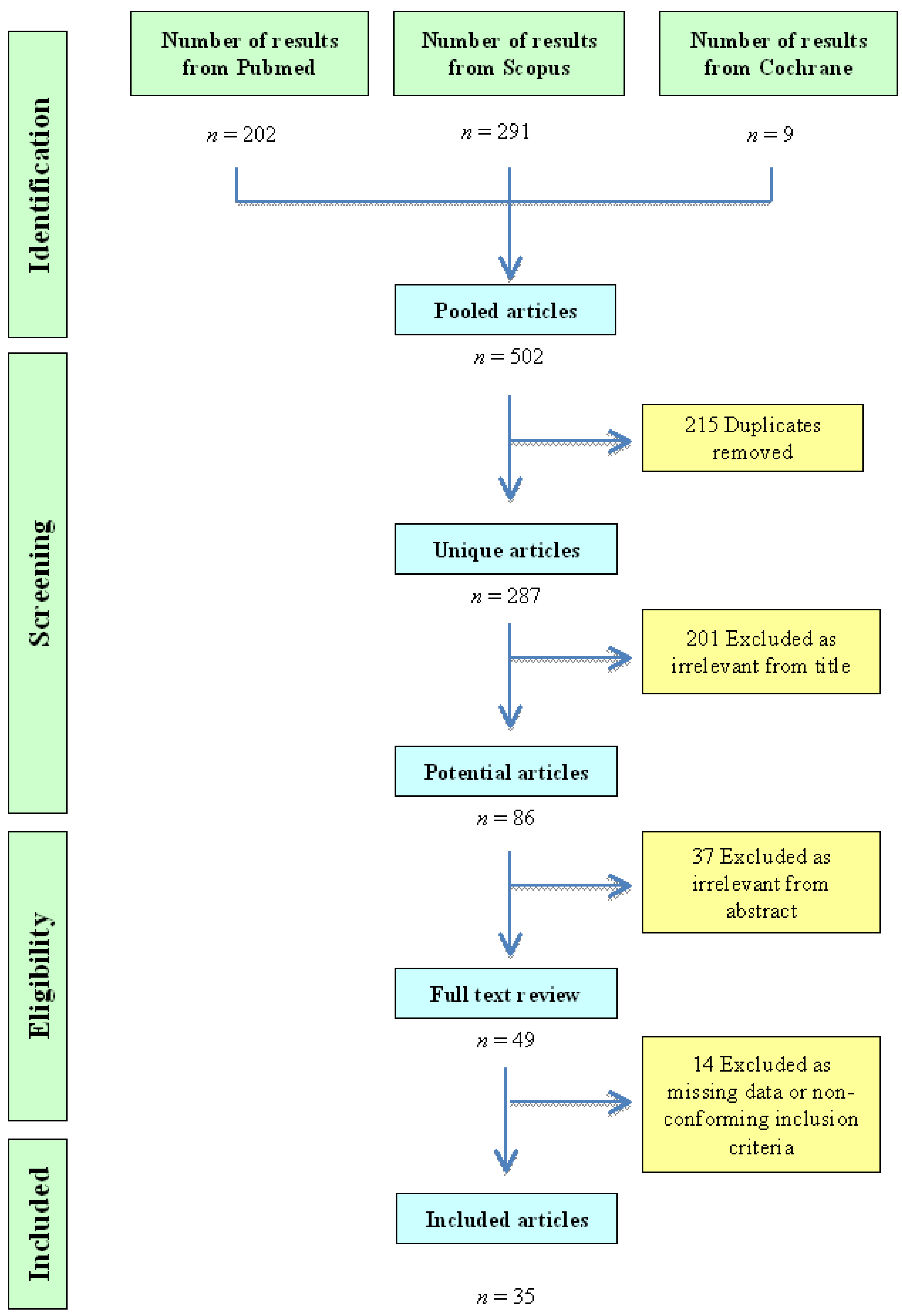
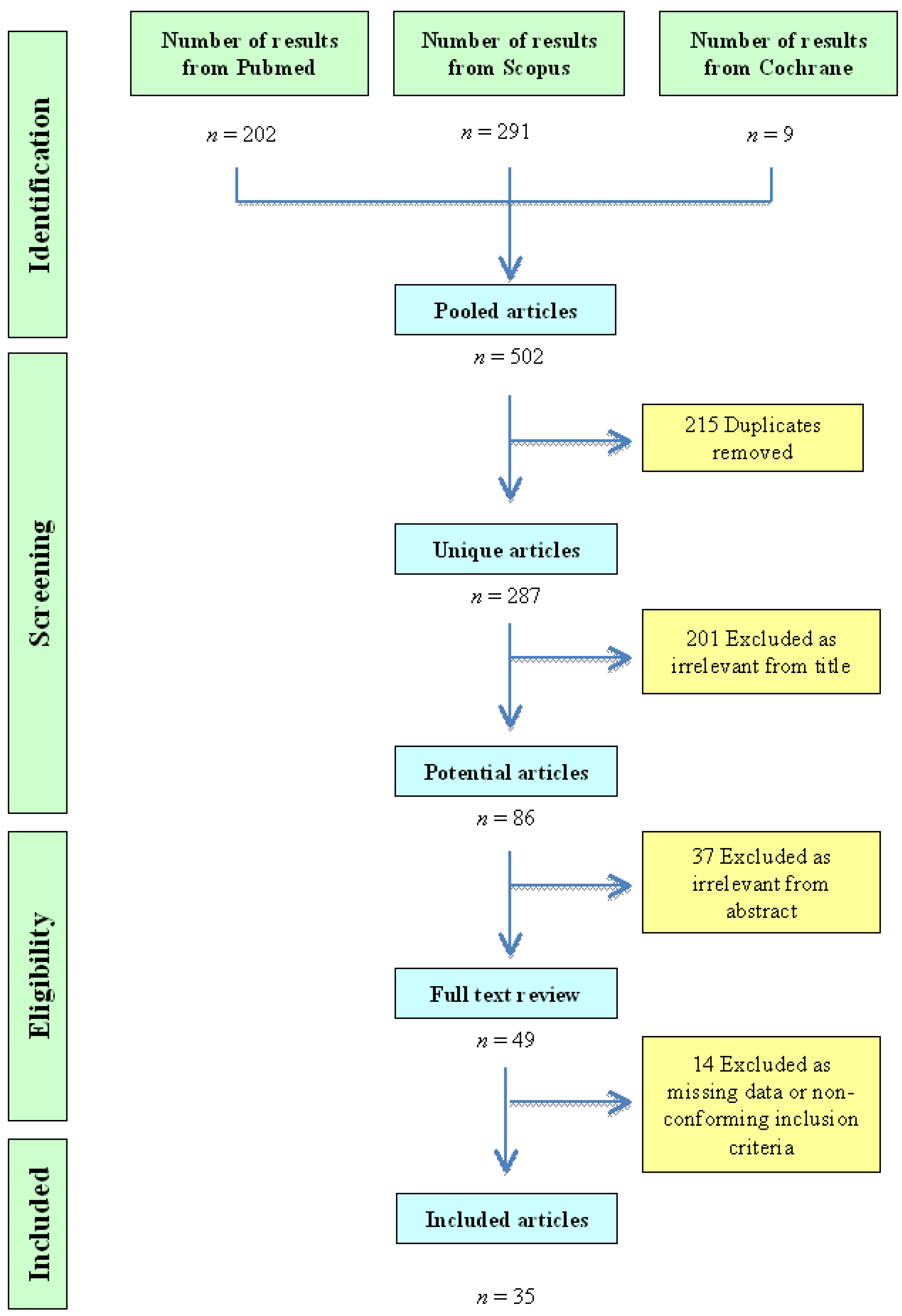
3.1. Identification of Studies
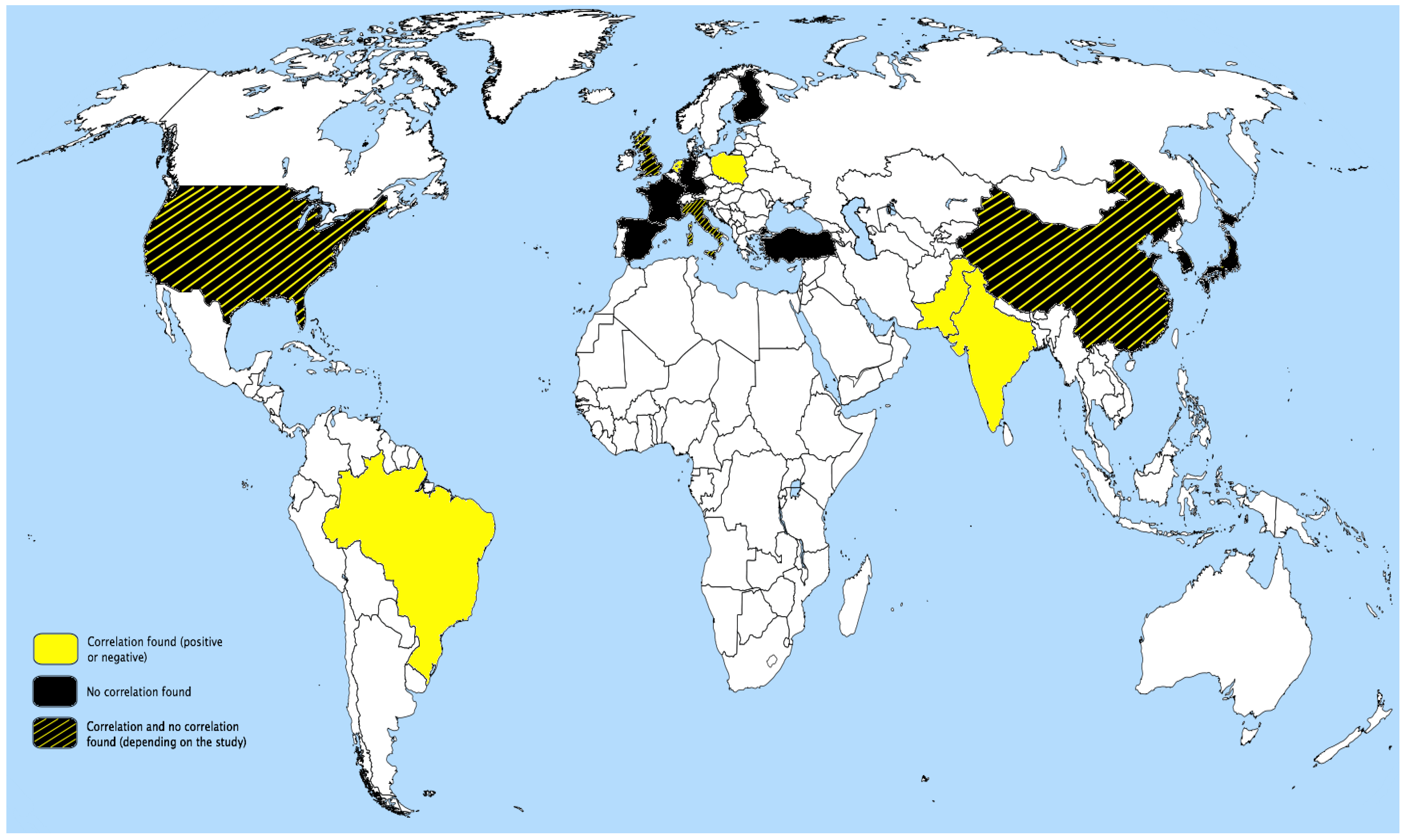
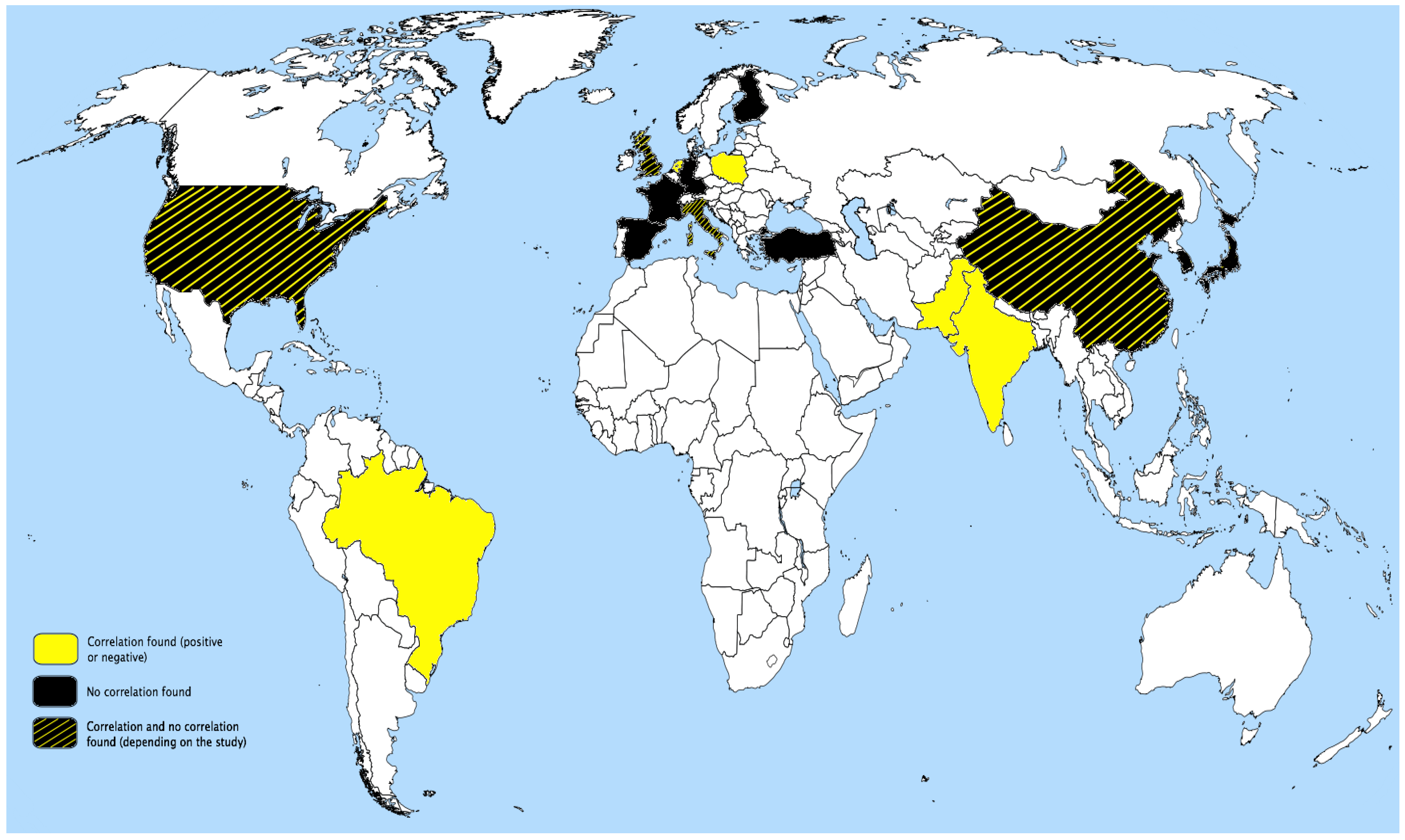
3.2. Study Characteristics

{kind=link}
{kind=link}
| First author | Year | Location of the studied population | Type of study | Patients (n) | Disease | Object of study | Enzyme activity measurement | Reference number | |
|---|---|---|---|---|---|---|---|---|---|
| GP | EA | ||||||||
| Liu, T. | 2014 | China | CC | 2456 | CAD | √ | √ | Paraoxonase-arylesterase | 13 |
| Shekhanawar, M. | 2013 | India | CS | 110 | CAD | - | √ | Arylesterase | 14 |
| Cozzi, L. | 2013 | Italy | CC | 105 | MI | √ | - | - | 15 |
| Tang, W.H.W. | 2012 | USA | C | 3668 | CAD MI | √ | √ | Paraoxonase-arylesterase | 16 |
| Bayrak, A. | 2012 | Turkey | CC | 270 | CAD | √ | √ | Thiolactonase-paraoxonase | 17 |
| Saxena, T. | 2011 | India | CC | 150 | MI | - | √ | Paraoxonase | 18 |
| Gluba, A. | 2010 | Poland | CC | 407 | MI | √ | - | - | 19 |
| Lakshmy, R. | 2010 | India | CC | 345 | MI | √ | √ | Paraoxonase | 20 |
| Regieli, J.J. | 2009 | Netherlands | C | 793 | CAD | √ | - | - | 21 |
| Jayakumari, N. | 2009 | India | CC | 574 | CAD | - | √ | Arylesterase | 22 |
| Yildiz, A. | 2008 | Turkey | CC | 134 | CAD | - | √ | Paraoxonase | 23 |
| Saeed, M. | 2007 | Pakistan | CC | 581 | MI | √ | - | - | 24 |
| Jarvik, G.P. | 2003 | USA | CC | 437 | CAD | √ | √ | Arylesterase | 25 |
| Domagala, T.B. | 2006 | U.K. | CC | 475 | CAD | √ | √ | Thiolactonase-paraoxonase | 26 |
| Su, S. | 2005 | China | CC | 423 | CAD | √ | √ | Arylesterase | 27 |
| Rodríguez-Esparragón, F. | 2005 | Spain | CC | 619 | CAD | √ | - | - | 28 |
| Kabarolgu, C. | 2004 | Turkey | CC | 103 | CAD MI | - | √ | Paraoxonase | 29 |
| Srinivasan, S.R. | 2004 | USA | C | 1786 | ATH | √ | - | - | 30 |
| Göçmen, A.Y. | 2004 | Turkey | CC | 172 | CAD | - | √ | Paraoxonase | 31 |
| Oliveira, S.A. | 2004 | Brazil | CC | 732 | CAD | √ | - | - | 32 |
| Robertson, K.S. | 2003 | U.K. | C | 3052 | CAD | √ | - | - | 33 |
| Wang, X. | 2003 | China | CC | 949 | CAD | √ | √ | Arylesterase | 34 |
| Fortunato, G. | 2003 | Italy | C | 310 | ATH | √ | - | - | 35 |
| Rahmani, M. | 2002 | Iran | CC | 251 | CAD | - | √ | Paraoxonase-arylesterase | 36 |
| Ferré, N. | 2002 | Spain | CC | 215 | MI | √ | √ | Paraoxonase | 37 |
| Hong, S.H. | 2001 | Korea | CC | 304 | CAD | √ | - | - | 38 |
| Malin, R. | 2001 | Finland | CS | 123 | ATH | √ | - | - | 39 |
| Gardemann, A. | 2000 | Germany | C | 2784 | CAD MI | √ | - | - | 40 |
| Cascorbi, I. | 1999 | Germany | CC | 2000 | CAD | √ | - | - | 41 |
| Sanghera, D.K. | 1998 | USA | CC | 318 | CAD MI | √ | - | - | 42 |
| Ombres, D. | 1998 | Italy | CC | 472 | CAD | √ | - | - | 43 |
| Sanghera, D.K. | 1997 | India-China | CC | 1034 | CAD | √ | - | - | 44 |
| Suehiro, T. | 1996 | Japan | CC | 386 | CAD MI | √ | - | - | 45 |
| Herrmann, S.M. | 1996 | France | CC | 1343 | MI | √ | - | - | 46 |
| McElveen, J. | 1986 | U.K. | CC | 283 | MI | - | √ | Paraoxonase | 47 |
3.3. PON Genetic Polymorphisms and CAD
3.4. PON1 Genetic Polymorphisms and Enzymatic Activity in CAD
3.5. PON1 Enzymatic Activity, Atherosclerosis and CAD
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Primo-Parmo, S.L.; Sorenson, R.C.; Teiber, J.; La Du, B.N. The human serum paraoxonase/arylesterase gene (PON1) is one member of a multigene family. Genomics 1996, 33, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Sorenson, R.C.; Primo-Parmo, S.L.; Camper, S.A.; La Du, B.N. The genetic mapping and gene structure of mouse paraoxonase/arylesterase. Genomics 1995, 30, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Gill, K.; Singh, S. Paraoxonases: structure, gene polymorphism & role in coronary artery disease. Indian J. Med. Res. 2009, 130, 361–368. [Google Scholar] [PubMed]
- Adkins, S.; Gan, K.N.; Mody, M.; La Du, B.N. Molecular basis for the polymorphic forms of human serum paraoxonase/arylesterase: glutamine or arginine at position 191, for the respective A or B allozymes. Am. J. Hum. Genet. 1993, 52, 598–608. [Google Scholar]
- She, Z.-G.; Chen, H.-Z.; Yan, Y.; Li, H.; Liu, D.-P. The human paraoxonase gene cluster as a target in the treatment of atherosclerosis. Antioxid. Redox Signal. 2012, 16, 597–632. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Marsillach, J.; Joven, J. The paraoxonases: role in human diseases and methodological difficulties in measurement. Crit. Rev. Clin. Lab. Sci. 2009, 46, 83–106. [Google Scholar] [CrossRef] [PubMed]
- Hine, D.; Mackness, B.; Mackness, M. Coincubation of PON1, APO A1, and LCAT increases the time HDL is able to prevent LDL oxidation. IUBMB Life. 2012, 64, 157–161. [Google Scholar] [CrossRef] [PubMed]
- Mackness, M.I.; Durrington, P.N.; Mackness, B. The role of paraoxonase 1 activity in cardiovascular disease: potential for therapeutic intervention. Am. J. Cardiovasc. Drugs. 2004, 4, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Mackness, M.I.; Mackness, B.; Durrington, P.N. Paraoxonase and coronary artery disease. Atheroscler. Suppl. 2002, 3, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Costa, L.G.; Giordano, G.; Cole, T.B.; Marsillach, J.; Furlong, C.E. Paraoxonase 1 (PON1) as a genetic determinant of susceptibility to organophosphate toxicity. Toxicology 2013, 307, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Khersonsky, O.; Tawfik, D.S. Structure-reactivity studies of serum paraoxonase PON1 suggest that its native activity is lactonase. Biochemistry 2005, 44, 6371–6382. [Google Scholar] [CrossRef] [PubMed]
- Khersonsky, O.; Tawfik, D.S. Chromogenic and fluorogenic assays for the lactonase activity of serum paraoxonases. Chembiochem. Eur. J. Chem. Biol. 2006, 7, 49–53. [Google Scholar] [CrossRef]
- Liu, T.; Zhang, X.; Zhang, J.; Liang, Z.; Cai, W.; Huang, M.; Yan, C.; Zhu, Z.; Han, Y. Association between PON1 rs662 polymorphism and coronary artery disease. Eur. J. Clin. Nutr. 2014, 68, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Shekhanawar, M.; Shekhanawar, S.M.; Krisnaswamy, D.; Indumati, V.; Satishkumar, D.; Vijay, V.; Rajeshwari, T.; Amareshwar, M. The role of “paraoxonase-1 activity” as an antioxidant in coronary artery diseases. J. Clin. Diagn. Res. JCDR 2013, 7, 1284–1287. [Google Scholar]
- Cozzi, L.; Campolo, J.; Parolini, M.; De Maria, R.; Patrosso, M.C.; Marocchi, A.; Parodi, O.; Penco, S. Paraoxonase 1 L55M, Q192R and paraoxonase 2 S311C alleles in atherothrombosis. Mol. Cell. Biochem. 2013, 374, 233–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, W.H.W.; Hartiala, J.; Fan, Y.; Wu, Y.; Stewart, A.F.R.; Erdmann, J.; Kathiresan, S.; CARDIoGRAM Consortium; Roberts, R.; McPherson, R.; Allayee, H.; Hazen, S.L. Clinical and genetic association of serum paraoxonase and arylesterase activities with cardiovascular risk. Arterioscler. Thromb. Vasc. Biol. 2012, 32, 2803–2812. [Google Scholar] [CrossRef] [PubMed]
- Bayrak, A.; Bayrak, T.; Tokgözoglu, S.L.; Volkan-Salanci, B.; Deniz, A.; Yavuz, B.; Alikasifoglu, M.; Demirpençe, E. Serum PON-1 activity but not Q192R polymorphism is related to the extent of atherosclerosis. J. Atheroscler. Thromb. 2012, 19, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Saxena, T; Agarwal, B.K.; Kare, P. Serum paraoxonase activity and oxidative stress in acute myocardial infarction patients. Biomed. Res. 2011, 22, 215–219. [Google Scholar]
- Gluba, A.; Pietrucha, T.; Banach, M.; Piotrowski, G.; Rysz, J. The role of polymorphisms within paraoxonases (192 Gln/Arg in PON1 and 311Ser/Cys in PON2) in the modulation of cardiovascular risk: a pilot study. Angiology 2010, 61, 157–165. [Google Scholar] [CrossRef] [PubMed]
- Lakshmy, R.; Ahmad, D.; Abraham, R.A.; Sharma, M.; Vemparala, K.; Das, S.; Reddy, K.S.; Prabhakaran, D. Paraoxonase gene Q192R & L55M polymorphisms in Indians with acute myocardial infarction & association with oxidized low density lipoprotein. Indian J. Med. Res. 2010, 131, 522–529. [Google Scholar]
- Regieli, J.J.; Jukema, J.W.; Doevendans, P.A.; Zwinderman, A.H.; Kastelein, J.J.; Grobbee, D.E.; van der Graaf, Y. Paraoxonase variants relate to 10-year risk in coronary artery disease: impact of a high-density lipoprotein-bound antioxidant in secondary prevention. J. Am. Coll. Cardiol. 2009, 54, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Jayakumari, N.; Thejaseebai, G. High prevalence of low serum paraoxonase-1 in subjects with coronary artery disease. J. Clin. Biochem. Nutr. 2009, 45, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Yildiz, A.; Gur, M.; Yilmaz, R.; Demirbag, R.; Polat, M.; Selek, S.; Celik, H.; Erel, O. Association of paraoxonase activity and coronary blood flow. Atherosclerosis 2008, 197, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Saeed, M.; Perwaiz Iqbal, M.; Yousuf, F.A.; Perveen, S.; Shafiq, M.; Sajid, J.; Frossard, P.M. Interactions and associations of paraoxonase gene cluster polymorphisms with myocardial infarction in a Pakistani population. Clin. Genet. 2007, 71, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Jarvik, G.P.; Hatsukami, T.S.; Carlson, C.; Richter, R.J.; Jampsa, R.; Brophy, VH.; Margolin, S.; Rieder, M.; Nickerson, D.; Schellenberg, G.D.; et al. Paraoxonase activity, but not haplotype utilizing the linkage disequilibrium structure, predicts vascular disease. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Domagała, T.B.; Łacinski, M.; Trzeciak, W.H.; Mackness, B.; Mackness, M.I.; Jakubowski, H. The correlation of homocysteine-thiolactonase activity of the paraoxonase (PON1) protein with coronary heart disease status. Cell. Mol. Biol. 2006, 52, 4–10. [Google Scholar] [PubMed]
- Su, S.; Chen, J.; Huang, J.; Wang, X.; Zhao, J.; Shen, Y.; Qiang, B.; Gu, D. Paraoxonase gene cluster variations associated with coronary heart disease in Chinese Han women. Chin. Med. J. (Engl.) 2005, 118, 1167–1174. [Google Scholar]
- Rodríguez-Esparragón, F.; Rodríguez-Pérez, J.C.; Hernández-Trujillo, Y.; Macías-Reyes, A.; Medina, A.; Caballero, A.; Ferrario, C.M. Allelic variants of the human scavenger receptor class B type 1 and paraoxonase 1 on coronary heart disease: genotype-phenotype correlations. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 854–860. [Google Scholar] [CrossRef] [PubMed]
- Kabaroglu, C.; Mutaf, I.; Boydak, B.; Ozmen, D.; Habif, S.; Erdener, D.; Parildar, Z.; Bayindir, O. Association between serum paraoxonase activity and oxidative stress in acute coronary syndromes. Acta. Cardiol. 2004, 59, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S.R.; Li, S.; Chen, W.; Tang, R.; Bond, M.G.; Boerwinkle, E.; Berenson, G.S. Q192R polymorphism of the paraoxanase 1 gene and its association with serum lipoprotein variables and carotid artery intima-media thickness in young adults from a biracial community. The Bogalusa Heart Study. Atherosclerosis 2004, 177, 167–174. [Google Scholar] [PubMed]
- Göçmen, A.Y.; Gümüşlü, S.; Semiz, E. Association between paraoxonase-1 activity and lipid peroxidation indicator levels in people living in the Antalya region with angiographically documented coronary artery disease. Clin. Cardiol. 2004, 27, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, S.A.; Mansur, A.P.; Ribeiro, C.C.; Ramires, J.A.F.; Annichino-Bizzacchi, J.M. PON1 M/L55 mutation protects high-risk patients against coronary artery disease. Int. J. Cardiol. 2004, 94, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Robertson, K.S.; Hawe, E.; Miller, G.J.; Talmud, P.J.; Humphries, S.E. Northwick Park Heart Study II Human paraoxonase gene cluster polymorphisms as predictors of coronary heart disease risk in the prospective Northwick Park Heart Study II. Biochim. Biophys. Acta 2003, 1639, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Fan, Z.; Huang, J.; Su, S.; Yu, Q.; Zhao, J.; Hui, R.; Yao, Z.; Shen, Y.; Qiang, B.; Gu, D. Extensive association analysis between polymorphisms of PON gene cluster with coronary heart disease in Chinese Han population. Arterioscler. Thromb. Vasc. Biol. 2003, 23, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Fortunato, G.; Rubba, P.; Panico, S.; Trono, D.; Tinto, N.; Mazzaccara, C.; de Michele, M.; Iannuzzi, A.; Vitale, D.F.; Salvatore, F.; et al. A paraoxonase gene polymorphism, PON 1 (55), as an independent risk factor for increased carotid intima-media thickness in middle-aged women. Atherosclerosis 2003, 167, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, M.; Raiszadeh, F.; Allahverdian, S.; Kiaii, S.; Navab, M.; Azizi, F. Coronary artery disease is associated with the ratio of apolipoprotein A-I/B and serum concentration of apolipoprotein B, but not with paraoxonase enzyme activity in Iranian subjects. Atherosclerosis 2002, 162, 381–389. [Google Scholar] [CrossRef] [PubMed]
- Ferré, N.; Tous, M.; Paul, A.; Zamora, A.; Vendrell, J.J.; Bardají, A.; Camps, J.; Richart, C.; Joven, J. Paraoxonase Gln-Arg(192) and Leu-Met(55) gene polymorphisms and enzyme activity in a population with a low rate of coronary heart disease. Clin. Biochem. 2002, 35, 197–203. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.H.; Song, J.; Min, W.K.; Kim, J.Q. Genetic variations of the paraoxonase gene in patients with coronary artery disease. Clin. Biochem. 2001, 34, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Malin, R.; Järvinen, O.; Sisto, T.; Koivula, T.; Lehtimäki, T. Paraoxonase producing PON1 gene M/L55 polymorphism is related to autopsy-verified artery-wall atherosclerosis. Atherosclerosis 2001, 157, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Gardemann, A.; Philipp, M.; Hess, K.; Katz, N.; Tillmanns, H.; Haberbosch, W. The paraoxonase Leu-Met54 and Gln-Arg191 gene polymorphisms are not associated with the risk of coronary heart disease. Atherosclerosis 2000, 152, 421–431. [Google Scholar] [CrossRef] [PubMed]
- Cascorbi, I.; Laule, M.; Mrozikiewicz, P.M.; Mrozikiewicz, A.; Andel, C.; Baumann, G.; Roots, I.; Stangl, K. Mutations in the human paraoxonase 1 gene: frequencies, allelic linkages, and association with coronary artery disease. Pharmacogenetics 1999, 9, 755–761. [Google Scholar] [PubMed]
- Sanghera, D.K.; Aston, C.E.; Saha, N.; Kamboh, M.I. DNA polymorphisms in two paraoxonase genes (PON1 and PON2) are associated with the risk of coronary heart disease. Am. J. Hum. Genet. 1998, 62, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Ombres, D.; Pannitteri, G.; Montali, A.; Candeloro, A.; Seccareccia, F.; Campagna, F.; Cantini, R.; Campa, P.P.; Ricci, G.; Arca, M. The gln-Arg192 polymorphism of human paraoxonase gene is not associated with coronary artery disease in Italian patients. Arterioscler. Thromb. Vasc. Biol. 1998, 18, 1611–1616. [Google Scholar] [CrossRef]
- Sanghera, D.K.; Saha, N.; Aston, C.E.; Kamboh, M.I. Genetic polymorphism of paraoxonase and the risk of coronary heart disease. Arterioscler. Thromb. Vasc. Biol. 1997, 17, 1067–1073. [Google Scholar] [CrossRef] [PubMed]
- Suehiro, T.; Nakauchi, Y.; Yamamoto, M.; Arii, K.; Itoh, H.; Hamashige, N.; Hashimoto, K. Paraoxonase gene polymorphism in Japanese subjects with coronary heart disease. Int. J. Cardiol. 1996, 57, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, S.M.; Blanc, H.; Poirier, O.; Arveiler, D.; Luc, G.; Evans, A.; Marques-Vidal, P.; Bard, J.M.; Cambien, F. The Gln/Arg polymorphism of human paraoxonase (PON 192) is not related to myocardial infarction in the ECTIM Study. Atherosclerosis 1996, 126, 299–303. [Google Scholar] [CrossRef] [PubMed]
- McElveen, J.; Mackness, M.I.; Colley, C.M.; Peard, T.; Warner, S.; Walker, C.H. Distribution of paraoxon hydrolytic activity in the serum of patients after myocardial infarction. Clin. Chem. 1986, 32, 671–673. [Google Scholar] [PubMed]
- Gaidukov, L.; Tawfik, D.S. The development of human sera tests for HDL-bound serum PON1 and its lipolactonase activity. J. Lipid Res. 2007, 48, 1637–1646. [Google Scholar] [CrossRef] [PubMed]
- Parra, S.; Marsillach, J.; Aragonès, G.; Rull, A.; Beltrán-Debón, R.; Alonso-Villaverde, C.; Joven, J.; Camps, J. Methodological constraints in interpreting serum paraoxonase-1 activity measurements: an example from a study in HIV-infected patients. Lipids Health Dis. 2010, 9. [Google Scholar] [CrossRef]
- Aviram, M.; Vaya, J. Paraoxonase 1 activities, regulation, and interactions with atherosclerotic lesion. Curr. Opin. Lipidol. 2013, 24, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Furlong, C.E.; Richter, R.J.; Li, W.F.; Brophy, V.H.; Carlson, C.; Rieder, M.; Nickerson, D.; Costa, L.G.; Ranchalis, J.; Lusis, A.J.; et al. The functional consequences of polymorphisms in the human PON1 gene. In The paraoxonases: Their Role in Disease Development and Xenobiotic Metabolism; Springer: Dordrecht, The Netherlands, 2008; Volume 6, pp. 267–281. [Google Scholar]
- Marsillach, J.; Aragonès, G.; Beltrán, R.; Caballeria, J.; Pedro-Botet, J.; Morcillo-Suárez, C.; Navarro, A.; Joven, J.; Camps, J. The measurement of the lactonase activity of paraoxonase-1 in the clinical evaluation of patients with chronic liver impairment. Clin. Biochem. 2009, 42, 91–98. [Google Scholar] [CrossRef] [PubMed]
- Camps, J.; Mackness, M.; Mackness, B.; Marsillach, J.; Joven, J. Serum paraoxonase-1 activity and genetic polymorphisms: common errors in measurement and interpretation of results. Clin. Chem. Lab. Med. 2010, 48, 893–894. [Google Scholar] [CrossRef] [PubMed]
- Marsillach, J.; Camps, J.; Beltran-Debón, R.; Rull, A.; Aragones, G.; Maestre-Martínez, C.; Sabench, F.; Hernández, M.; Castillo, D.D.; Joven, J.; et al. Immunohistochemical analysis of paraoxonases-1 and 3 in human atheromatous plaques. Eur. J. Clin. Invest. 2011, 41, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Fortunato, G.; Di Taranto, M.D.; Bracale, U.M.; Del Guercio, L.; Carbone, F.; Mazzaccara, C.; Morgante, A.; D’Armiento, F.P.; D’Armiento, M.; Porcellini, M.; et al. Decreased paraoxonase-2 expression in human carotids during the progression of atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Tavori, H.; Vaya, J.; Aviram, M. Paraoxonase 1 attenuates human plaque atherogenicity: relevance to the enzyme lactonase activity. Adv. Exp. Med. Biol. 2010, 660, 99–111. [Google Scholar] [PubMed]
- Martinelli, N.; Consoli, L.; Girelli, D.; Grison, E.; Corrocher, R.; Olivieri, O. Paraoxonases: ancient substrate hunters and their evolving role in ischemic heart disease. Adv. Clin. Chem. 2013, 59, 65–100. [Google Scholar] [PubMed]
- Liu, H.; Xia, P.; Liu, M.; Ji, X.M.; Sun, H.B.; Tao, L.; Mu, Q.W. PON gene polymorphisms and ischaemic stroke: a systematic review and meta analysis. Int. J. Stroke 2013, 8, 111–123. [Google Scholar] [CrossRef] [PubMed]
- Précourt, L.-P.; Amre, D.; Denis, M.-C.; Lavoie, J.-C.; Delvin, E.; Seidman, E.; Levy, E. The three-gene paraoxonase family: physiologic roles, actions and regulation. Atherosclerosis 2011, 214, 20–36. [Google Scholar] [CrossRef] [PubMed]
- Ng, C.J.; Shih, D.M.; Hama, S.Y.; Villa, N.; Navab, M.; Reddy, S.T. The paraoxonase gene family and atherosclerosis. Free Radic. Biol. Med. 2005, 38, 153–163. [Google Scholar] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abelló, D.; Sancho, E.; Camps, J.; Joven, J. Exploring the Role of Paraoxonases in the Pathogenesis of Coronary Artery Disease: A Systematic Review. Int. J. Mol. Sci. 2014, 15, 20997-21010. https://doi.org/10.3390/ijms151120997
Abelló D, Sancho E, Camps J, Joven J. Exploring the Role of Paraoxonases in the Pathogenesis of Coronary Artery Disease: A Systematic Review. International Journal of Molecular Sciences. 2014; 15(11):20997-21010. https://doi.org/10.3390/ijms151120997
Chicago/Turabian StyleAbelló, David, Elena Sancho, Jordi Camps, and Jorge Joven. 2014. "Exploring the Role of Paraoxonases in the Pathogenesis of Coronary Artery Disease: A Systematic Review" International Journal of Molecular Sciences 15, no. 11: 20997-21010. https://doi.org/10.3390/ijms151120997