Clinicopathological Significance of Loss of ARID1A Immunoreactivity in Ovarian Clear Cell Carcinoma

Abstract
:1. Introduction
2. Results and Discussion
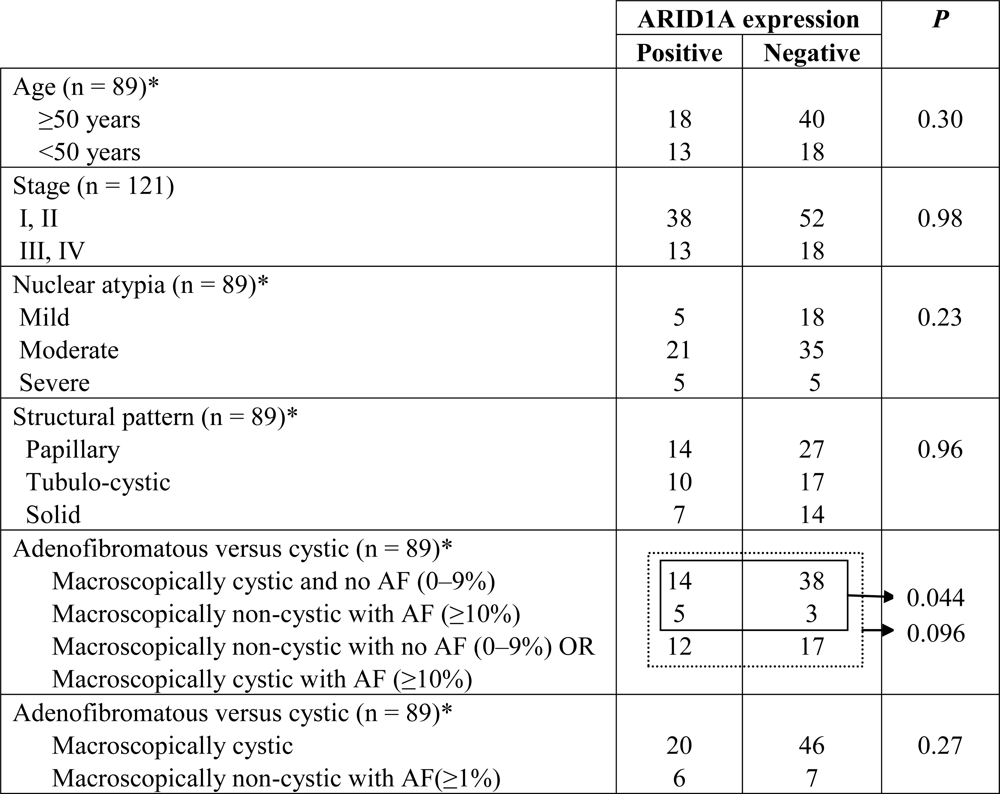
2.1. Results
2.2. Discussion
3. Experimental Section
3.1. Tissue Materials
3.2. Immunohistochemistry
3.3. Statistical Analysis
4. Conclusion
Acknowledgments
References
- Jones, S; Wang, TL; Shih, IM; Mao, TL; Nakayama, K; Roden, R; Glas, R; Slamon, D; Diaz, L; Vogelstein, B; et al. Frequent mutations of chromatin remodeling gene ARID1A in ovarian clear cell carcinoma. Science 2010, 330, 228–231. [Google Scholar]
- Wiegand, KC; Shah, SP; Al-Agha, OM; Zhao, Y; Tse, K; Zeng, T; Senz, J; McConechy, M; Anglesio, MS; Kalloger, SE; et al. ARID1A mutations in endometriosis-associated ovarian carcinomas. N. Engl. J. Med 2010, 363, 1532–1543. [Google Scholar]
- Kuo, K; Mao, T; Feng, Y; Feng, Y; Nakayama, K; Wang, Y; Glas, R; Ma, J; Kurman, RJ; Shih, IM; et al. DNA copy number profiles in affinity-purified ovarian clear cell carcinoma. Clin. Cancer Res 2010, 16, 1997–2008. [Google Scholar]
- Wang, X; Nagl, NG; Wilsker, D; van Scoy, M; Pacchione, S; Yaciuk, P; Dallas, PB; Moran, E. Two related ARID family proteins are alternative subunits of human SWI/SNF complexes. Biochem. J 2004, 383, 319–325. [Google Scholar]
- Ho, L; Crabtree, GR. Chromatin remodelling during development. Nature 2010, 463, 474–484. [Google Scholar]
- van Rechem, C; Boulay, G; Leprince, D. HIC1 interacts with a specific subunit of SWI/SNF complexes, ARID1A/BAF250A. Biochem. Biophys. Res. Commun 2009, 385, 586–590. [Google Scholar]
- Reisman, D; Glaros, S; Thompson, EA. The SWI/SNF complex and cancer. Oncogene 2009, 28, 1653–1668. [Google Scholar]
- Gao, X; Tate, P; Hu, P; Tjian, R; Skarnes, WC; Wang, Z. ES cell pluripotency and germ-layer formation require the SWI/SNF chromatin remodeling component BAF250a. Proc. Natl. Acad. Sci. USA 2008, 105, 6656–6661. [Google Scholar]
- Nagl, NG, Jr; Patsialou, A; Haines, DS; Dallas, PB; Beck, GR; Moran, E. The p270 (ARID1A/SMARCF1) subunit of mammalian SWI/SNF-related complexes is essential for normal cell cycle arrest. Cancer Res 2005, 65, 9236–9244. [Google Scholar]
- Huang, J; Zhao, YL; Li, Y; Fletcher, JA; Xian, S. Genomic and functional evidence for an ARID1A tumor suppressor role. Genes Chrom. Cancer 2007, 46, 745–750. [Google Scholar]
- Veras, E; Mao, TL; Ayhan, A; Ueda, S; Lai, H; Shih, IM; Kurman, RJ. Cystic and adenofibromatous clear cell carcinomas of the ovary: distinctive tumors that differ in their pathogenesis and behavior: A clinicopathologic analysis of 122 cases. Am. J. Surg. Pathol 2009, 33, 844–853. [Google Scholar]

{kind=link}
{kind=link}
| Immunostaining intensity score | Number of cases | |
|---|---|---|
| 0 | 88 | Negative, n = 88 |
| 1+ | 36 | ] Positive, n = 61 |
| 2+ | 25 | |
| Total | 149 | |
| Staining intensity score | Adnexal endometriosis | Endometrium Proliferative | Endometrium Secretory | Endometrium Menstrual | Endometrium Gestational |
|---|---|---|---|---|---|
| 0 | 0 | 0 | 0 | 0 | 0 |
| 1+ | 3 | 0 | 2 | 2 | 6 |
| 2+ | 2 | 11 | 9 | 2 | 6 |
| Total | 5 | 11 | 11 | 4 | 12 |
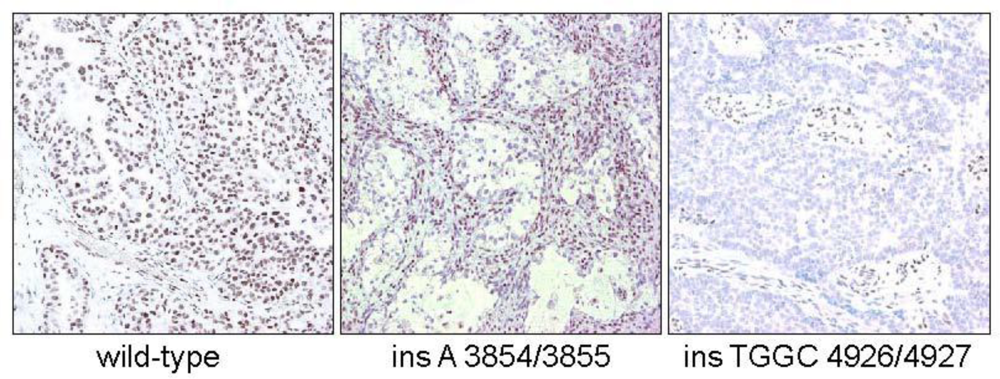
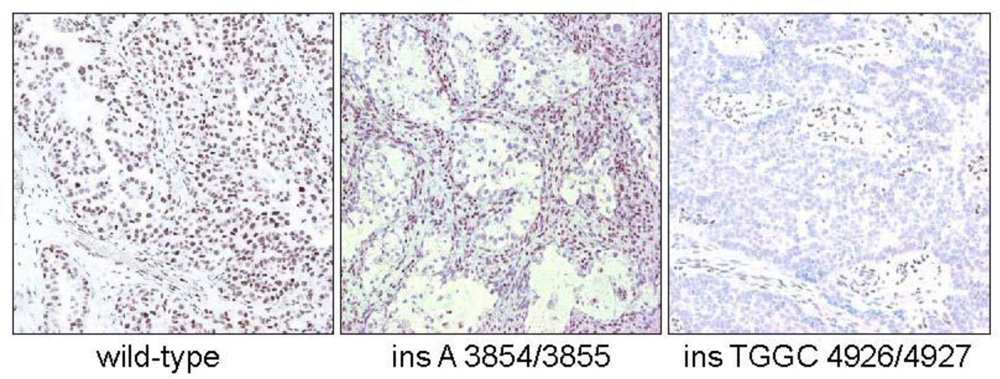
| Mutant | Wild-type | |
|---|---|---|
| IHC+ | 0 | 2 |
| IHC− | 9 | 1 |
© 2010 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Maeda, D.; Mao, T.-L.; Fukayama, M.; Nakagawa, S.; Yano, T.; Taketani, Y.; Shih, I.-M. Clinicopathological Significance of Loss of ARID1A Immunoreactivity in Ovarian Clear Cell Carcinoma. Int. J. Mol. Sci. 2010, 11, 5120-5128. https://doi.org/10.3390/ijms11125120
Maeda D, Mao T-L, Fukayama M, Nakagawa S, Yano T, Taketani Y, Shih I-M. Clinicopathological Significance of Loss of ARID1A Immunoreactivity in Ovarian Clear Cell Carcinoma. International Journal of Molecular Sciences. 2010; 11(12):5120-5128. https://doi.org/10.3390/ijms11125120
Chicago/Turabian StyleMaeda, Daichi, Tsui-Lien Mao, Masashi Fukayama, Shunsuke Nakagawa, Tetsu Yano, Yuji Taketani, and Ie-Ming Shih. 2010. "Clinicopathological Significance of Loss of ARID1A Immunoreactivity in Ovarian Clear Cell Carcinoma" International Journal of Molecular Sciences 11, no. 12: 5120-5128. https://doi.org/10.3390/ijms11125120