
Contact-Free Detection of Obstructive Sleep Apnea Based on Wavelet Information Entropy Spectrum Using Bio-Radar


Abstract
:1. Introduction
2. Materials and Methods
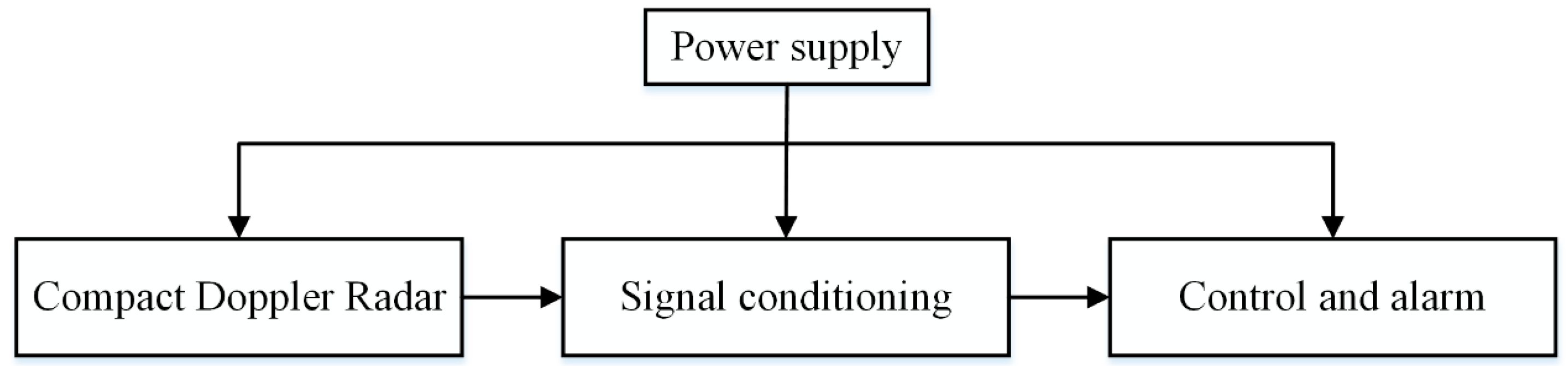
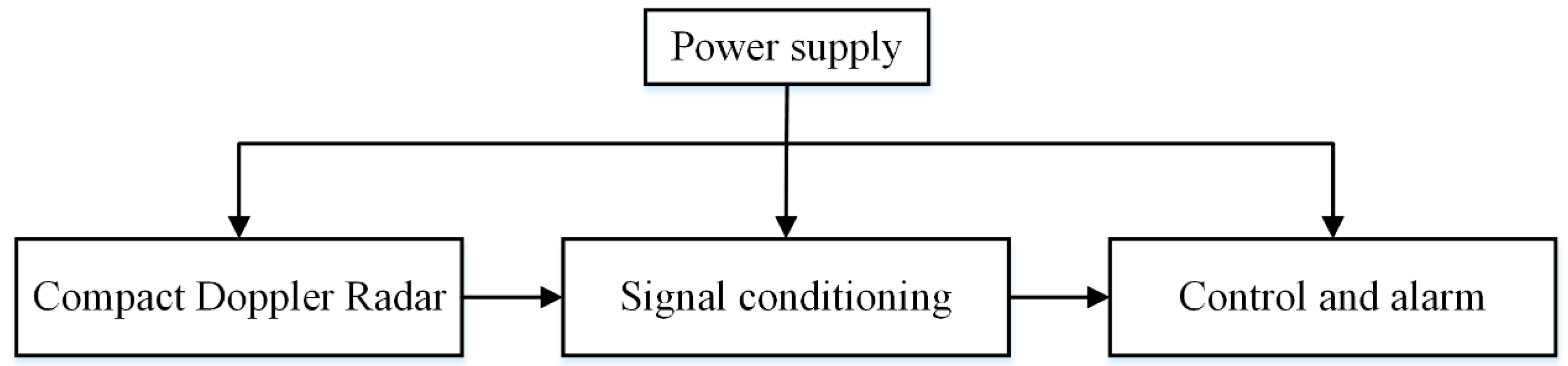
2.1. Description of Bio-Radar System for Detection of OSA
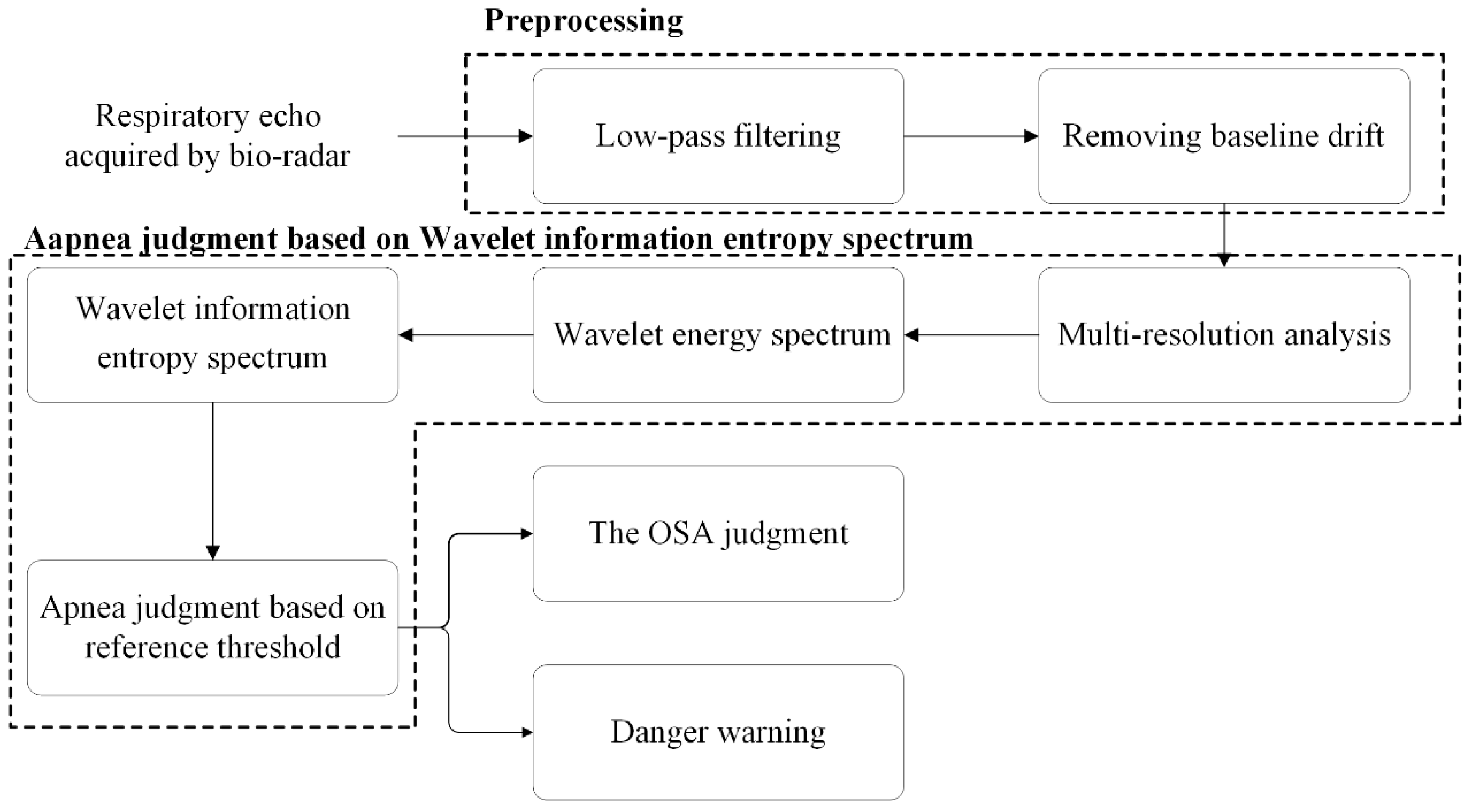
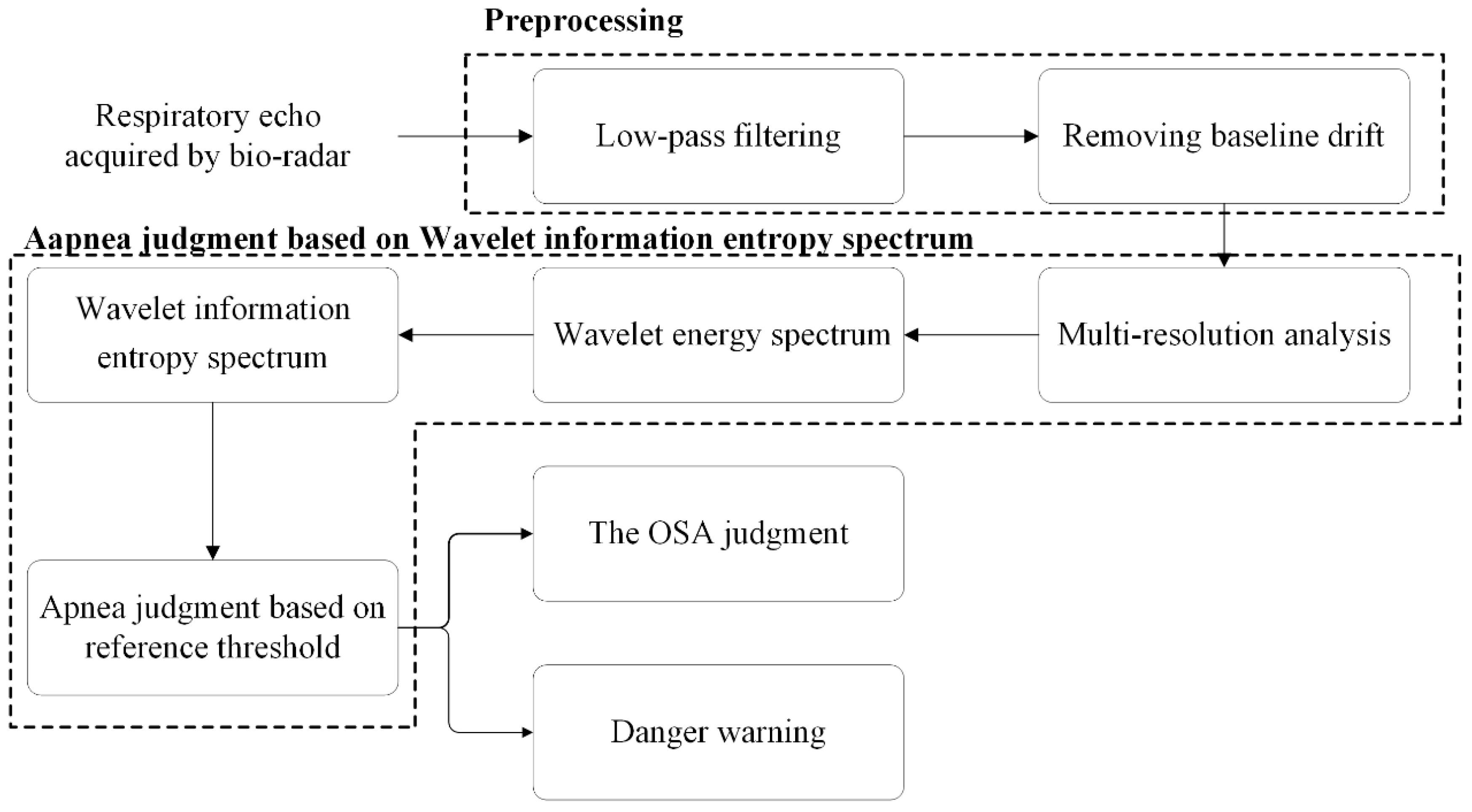
2.2. Apnea Detection Method
2.2.1. Signal Preprocessing
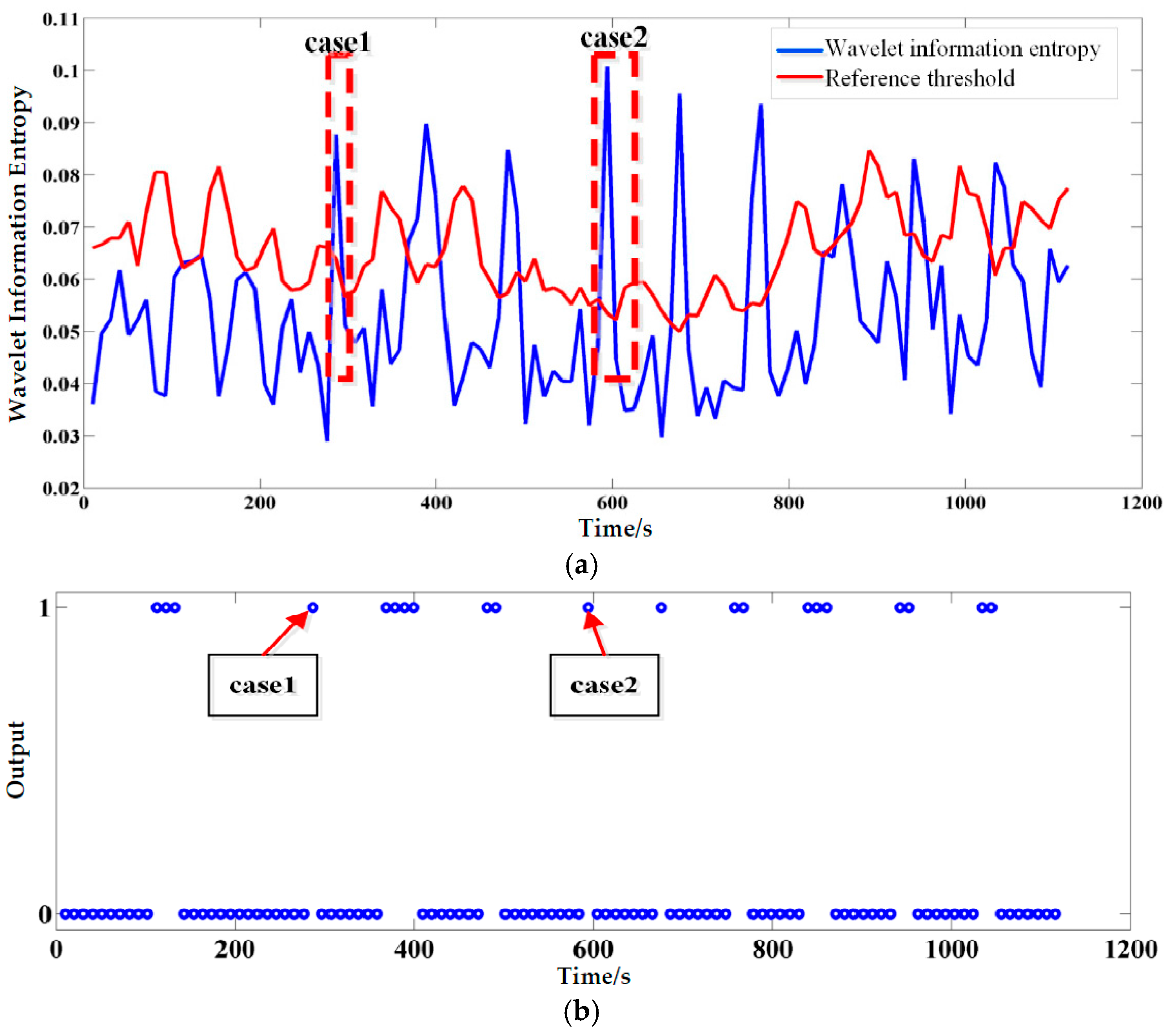
2.2.2. Wavelet Information Entropy
- (a)
- Selection of Mother Wavelet
- (b)
- Wavelet Information Entropy Spectrum
2.2.3. OSA Syndrome Judgment and Danger Warning
- (a)
- The OSA Syndrome Judgment
- (b)
- Danger Warning
3. Results
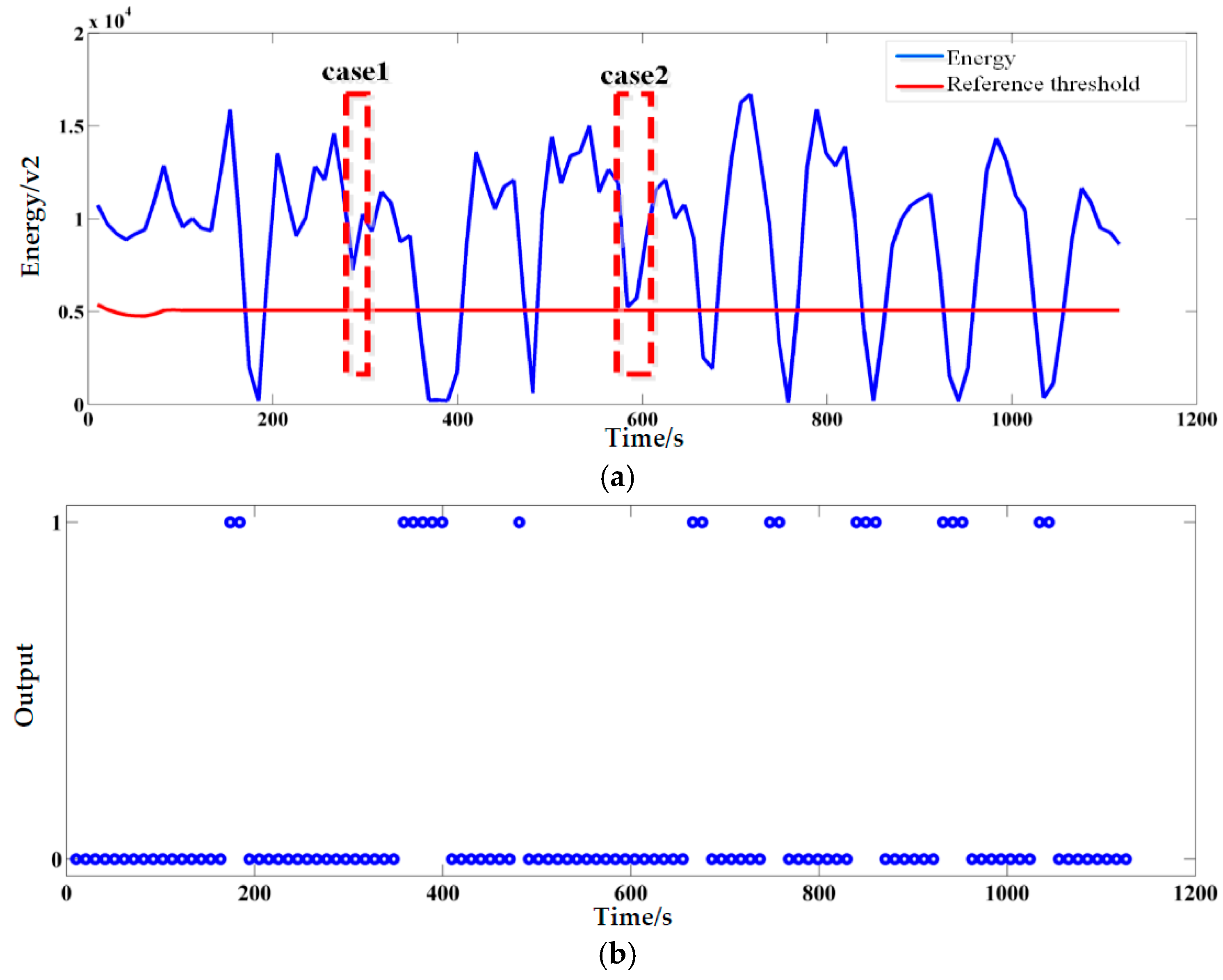
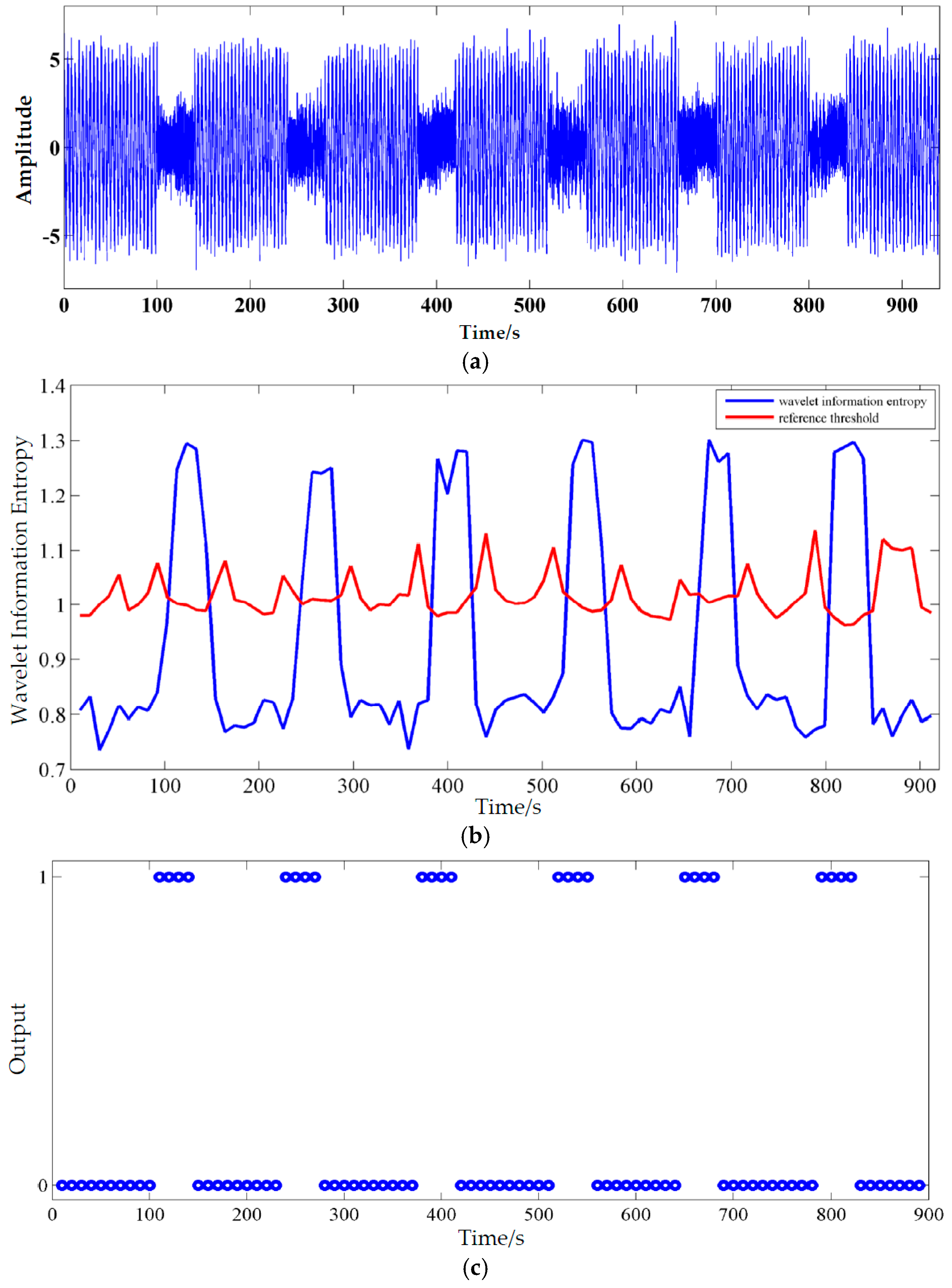
3.1. Simulation Results
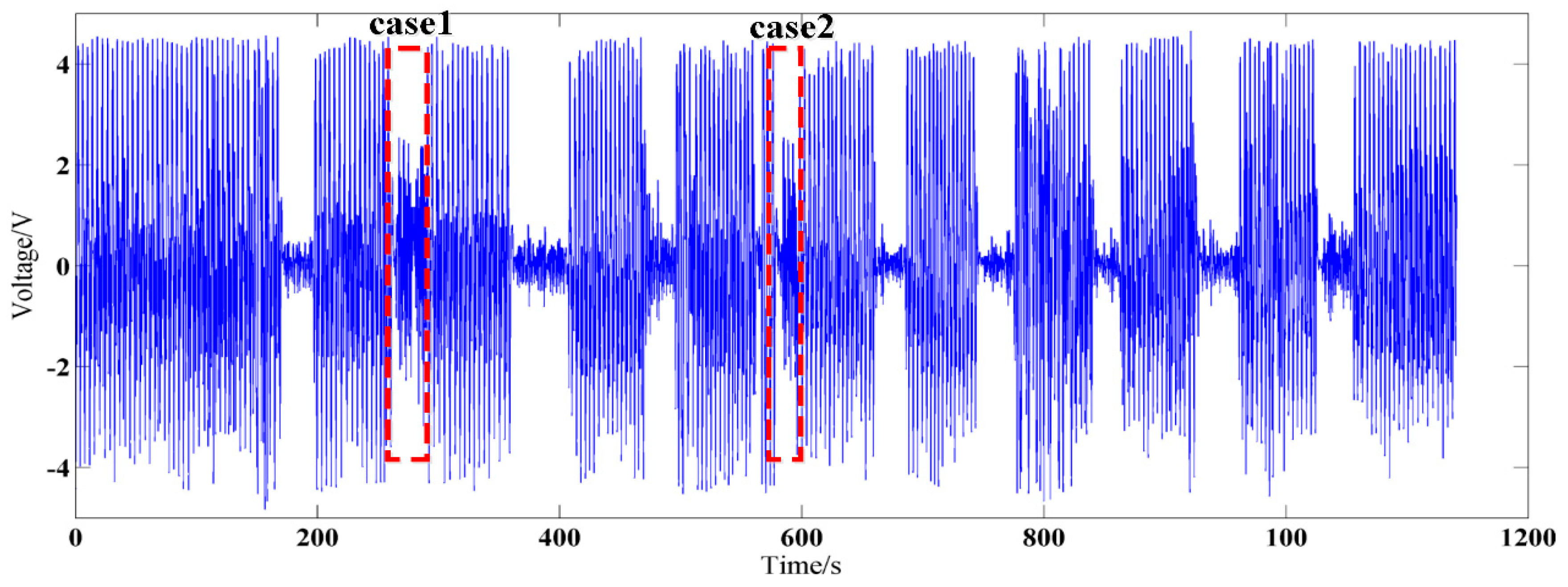
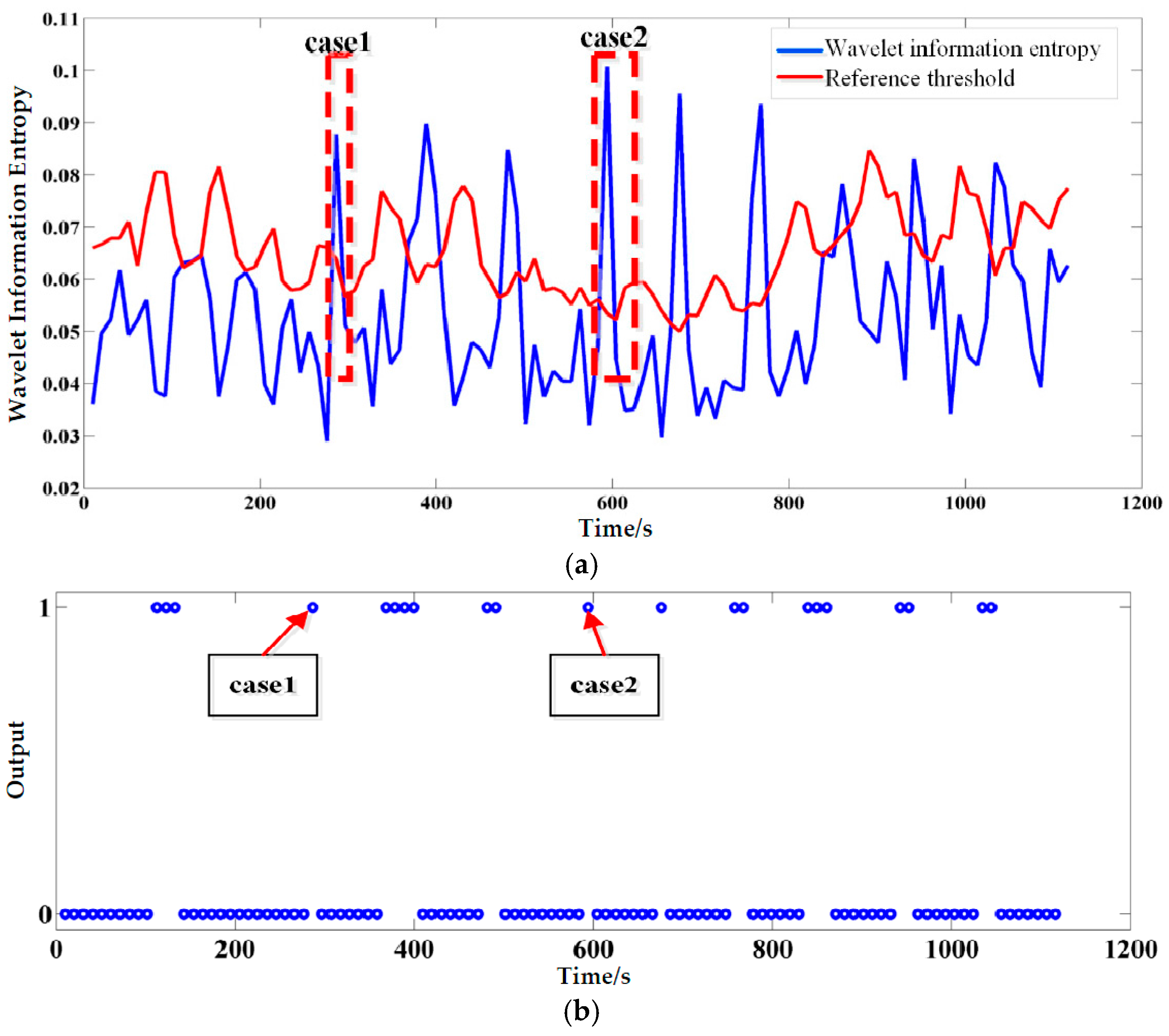
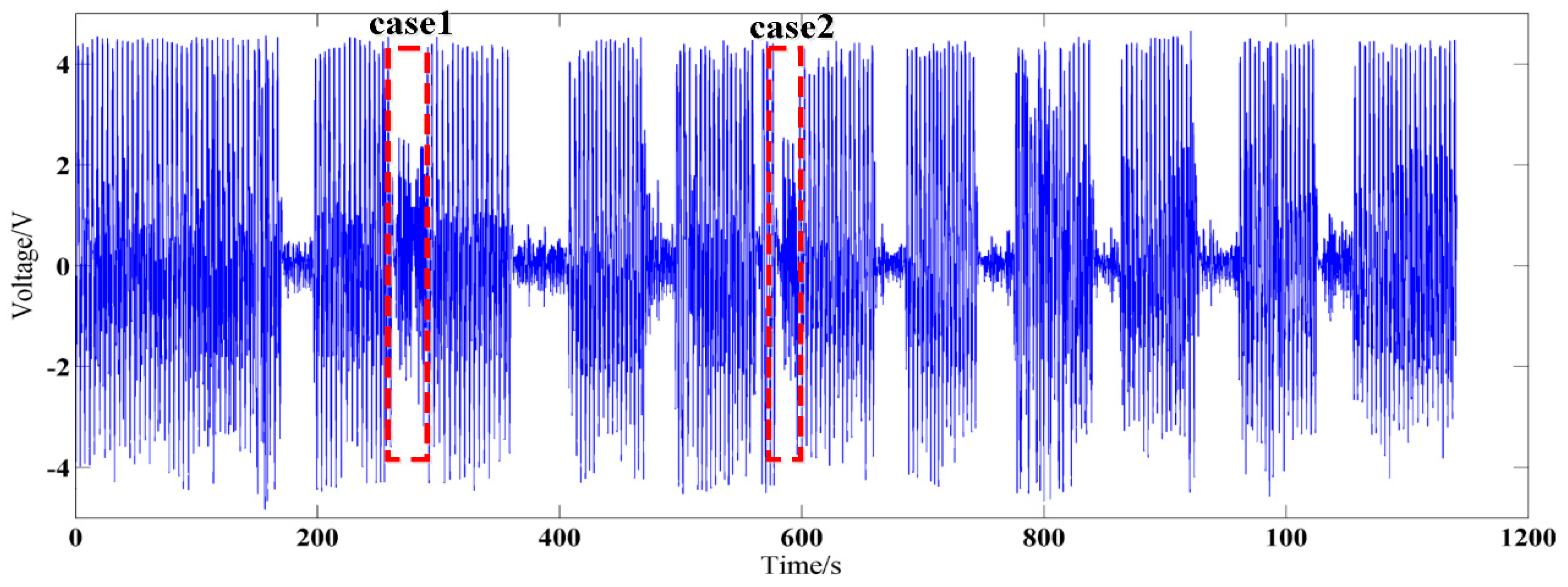
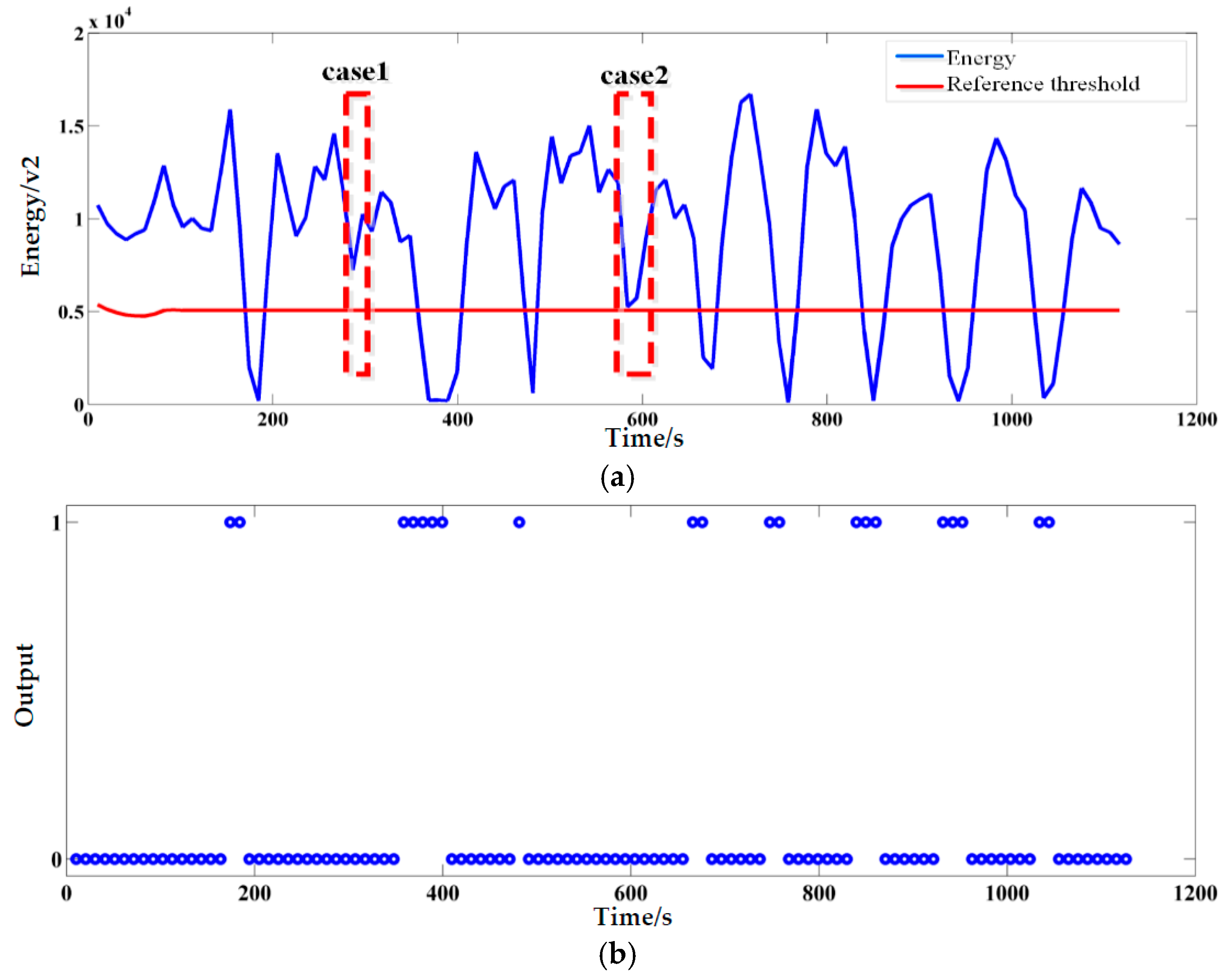
3.2. The Processing Results of Actual OSA Signals Acquired by Radar
3.3. The Judging Accuracy of the Proposed Method
4. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Mannarino, M.R.; di Filippo, F.; Pirro, M. Obstructive sleep apnea syndrome. Eur. J. Int. Med. 2012, 23, 586–593. [Google Scholar] [CrossRef] [PubMed]
- Guilleminault, C. Obstructive sleep apnea syndrome. In Sleep Disorders Medicine: Basic Science, Technical Considerations, and Clinical Aspects; Chokroverty, S., Ed.; Butterworth-Heinemann: Oxford, UK, 1994; pp. 199–217. [Google Scholar]
- Young, T.; Evans, L.; Finn, L.; Palta, M. Estimation of the clinically diagnosed proportion of sleep apnea syndrome in middle-aged men and women. Sleep 1997, 20, 705–706. [Google Scholar] [PubMed]
- Marshall, N.S.; Wong, K.K.; Liu, P.Y.; Cullen, S.R.; Knuiman, M.W.; Grunstein, R.R. Sleep Apnea as an Independent Risk Factor for All-Cause Mortality: The Busselton Health Study. Sleep 2008, 31, 1079–1085. [Google Scholar] [PubMed]
- Burwell, C.S.; Robin, E.D.; Whaley, R.D.; Bickelmann, A.G. Extreme obesity associated with alveolar hypoventilation—A Pickwickian syndrome. Am. J. Med. 1956, 21, 811–818. [Google Scholar] [CrossRef]
- Quan, S.; Gillin, J.C.; Littner, M.; Shepard, J. Sleep-related breathing disorders in adults: Recommendations for syndrome definition and measurement techniques in clinical research. editorials. Sleep 1999, 22, 662–689. [Google Scholar] [PubMed]
- Stradling, J.R.; Davies, R.J.O. Sleep 1: Obstructive sleep apnoea/hypopnoea syndrome: Definitions, epidemiology, and natural history. Thorax 2004, 59, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Lettieri, C.J.; Eliasson, A.H.; Andrada, T.; Khramtsov, A.; Raphaelson, M.; Kristo, D.A. Obstructive sleep apnea syndrome: Are we missing an at-risk population? CHEST J. 2005, 128. [Google Scholar] [CrossRef]
- Várady, P.; Micsik, T.; Benedek, S.; Benyó, Z. A novel method for the detection of apnea and hypopnea events in respiration signals. IEEE Trans. Biomed. Eng. 2002, 49, 936–942. [Google Scholar] [CrossRef] [PubMed]
- Yuan, G.; Drost, N.A.; McIvor, R.A. Respiratory rate and breathing pattern. McMaster Univ. Med. J. 2013, 10, 23–25. [Google Scholar]
- Sanders, M.; Costantino, J.; Strollo, P.; Studnicki, K.; Atwood, C. The impact of split-night polysomnography for diagnosis and positive pressure therapy titration on treatment acceptance and adherence in sleep apnea/hypopnea. Sleep 2000, 23, 17–24. [Google Scholar]
- Hedner, J.; Pillar, G.; Pittman, S.D.; Zou, D.; Grote, L.; White, D.P. A novel adaptive wrist actigraphy algorithm for sleep-wake assessment in sleep apnea patients. Sleep 2004, 27, 1560–1566. [Google Scholar] [PubMed]
- Vaughn, C.M.; Clemmons, P. Piezoelectric belts as a method for measuring chest and abdominal movement for obstructive sleep apnea diagnosis. Neurodiagn. J. 2012, 52, 275–280. [Google Scholar] [PubMed]
- Pereira, C.B.; Yu, X.; Czaplik, M.; Rossaint, R.; Blazek, V.; Leonhardt, S. Remote monitoring of breathing dynamics using infrared thermography. Biomed. Opt. Express 2015, 6, 4378–4394. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Jing, X.; Jiao, T.; Zhang, Z.; Lv, H.; Wang, J. Detecting and identifying two stationary-human-targets: A technique based on bioradar. In Proceedings of the First International Conference on Pervasive Computing Signal Processing and Applications (PCSPA), Harbin, China, 17–19 September 2010; pp. 981–985.
- Lee, Y.S.; Pathirana, P.N.; Caelli, T.; Evans, R. Doppler radar in respiratory monitoring: Detection and analysis. In Proceedings of the International Conference on Control, Automation and Information Sciences (ICCAIS), Nha Trang, Vietnam, 25–28 November 2013; pp. 224–228.
- Kagawa, M.; Tojima, H.; Matsui, T. Non-contact screening system for sleep apnea-hypopnea syndrome using the time-varying baseline of radar amplitudes. In Proceedings of the IEEE Healthcare Innovation Conference (HIC), Seattle, WA, USA, 8–10 October 2014; pp. 99–102.
- Zhang, P.-F.; Jing, X.-J.; Zhang, H.; Lu, G.-H.; Wang, J.-Q. Study on Technique for Non-contact Apnea Detection Based on Energy Spectrum. Chin. Med. Equip. J. 2012, 33, 13–15. [Google Scholar]
- Tagluk, M.E.; Sezgin, N. Classification of sleep apnea through sub-band energy of abdominal effort signal using wavelets + neural networks. J. Med. Syst. 2010, 34, 1111–1119. [Google Scholar] [CrossRef] [PubMed]
- Sezgin, N.; Tagluk, M.E. Energy based feature extraction for classification of sleep apnea syndrome. Comput. Biol. Med. 2009, 39, 1043–1050. [Google Scholar] [CrossRef] [PubMed]
- Alekhin, M.; Anishchenko, L.; Zhuravlev, A. Artificial neural networks and wavelet analysis in bio-radiolocation signal breathing patterns classification. In Proceedings of the 7th Russian Bavarian Conference, Erlangen, Germany, 10–14 October 2011.
- Lu, G.; Yang, F.; Tian, Y.; Jing, X.; Wang, J. Contact-free measurement of heart rate variability via a microwave sensor. Sensors 2009, 9, 9572–9581. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.C.; Zeng, Z.; Lai, P.; Feng, H.; Jin, S.-J. A recognition method with wavelet energy spectrum and wavelet information entropy for abnormal vibration events of a petroleum pipeline. J. Vib. Shock 2010, 29, 1–5. (In Chinese) [Google Scholar]
- Al-Nashash, H.; Thakor, N.V. Monitoring of global cerebral ischemia using wavelet entropy rate of change. IEEE Trans. Biomed. Eng. 2005, 52, 2119–2122. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Y.; Roberge, D.; Szu, H.H. Optical wavelet transform. Opt. Eng. 1992, 31, 1840–1845. [Google Scholar] [CrossRef]
- Jawerth, B.; Sweldens, W. An overview of wavelet based multiresolution analyses. SIAM Rev. 1994, 36, 377–412. [Google Scholar] [CrossRef]
- Chesson, A.; Ferber, R.A.; Fry, J.M.; Grigg-Damberger, M.; Hartse, K.; Hurwitz, T.; Johnson, S.; Littner, M.; Kader, G.; Rosen, G. Practice parameters for the indications for polysomnography and related procedures. Sleep 1997, 20, 406–422. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Result Number | PSG System (time) | Bio-Radar System (time) | Accuracy (%) |
|---|---|---|---|
| 1 | 20 | 19 | 95.0% |
| 2 | 23 | 21 | 91.3% |
| 3 | 10 | 10 | 100% |
| 4 | 26 | 24 | 92.3% |
| 5 | 20 | 22 | 90.0% |
| 6 | 19 | 20 | 94.7% |
| 7 | 13 | 15 | 84.6% |
| 8 | 17 | 18 | 94.1% |
| 9 | 23 | 22 | 95.7% |
| 10 | 29 | 27 | 93.1% |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, F.; Li, C.; Wang, S.; Zhang, H.; Wang, J.; Lu, G. Contact-Free Detection of Obstructive Sleep Apnea Based on Wavelet Information Entropy Spectrum Using Bio-Radar. Entropy 2016, 18, 306. https://doi.org/10.3390/e18080306
Qi F, Li C, Wang S, Zhang H, Wang J, Lu G. Contact-Free Detection of Obstructive Sleep Apnea Based on Wavelet Information Entropy Spectrum Using Bio-Radar. Entropy. 2016; 18(8):306. https://doi.org/10.3390/e18080306
Chicago/Turabian StyleQi, Fugui, Chuantao Li, Shuaijie Wang, Hua Zhang, Jianqi Wang, and Guohua Lu. 2016. "Contact-Free Detection of Obstructive Sleep Apnea Based on Wavelet Information Entropy Spectrum Using Bio-Radar" Entropy 18, no. 8: 306. https://doi.org/10.3390/e18080306