1. Introduction
For a long time surface electromyography (EMG) signals have been used for myoelectric prosthesis control for individuals with limb amputation [
1]. Proportional myoelectric control is the most popular control scheme used in clinical practice. Proportional control refers to the fact that the speed or force of the prosthesis is proportionally driven by the intensity of the EMG signal [
2]. Various parameters have been used to estimate the EMG intensity for implementing proportional myoelectric control, and the majority of these parameters are associated with amplitude measurements, such as the averaged rectified value (ARV), the root mean square (RMS) amplitude, and the waveform length (WL) of a surface EMG signal [
1,
2]. One limitation of such parameters associated with signal amplitude is that they are susceptible to different kinds of noise that may contaminate the surface EMG signals.
When recording surface EMG from muscles in the torso of the body, a typical noise that may contaminate surface EMG signals is the cardiac activity (electrocardiography, ECG) produced by the heart [
3,
4,
5,
6,
7]. This has become a major barrier to proportional control of myoelectric prosthesis using a novel neural machine interface called targeted muscle reinnervation (TMR). The TMR surgery technique involves transferring an amputee’s residual nerves to nonfunctional muscles toward enhancement of myoelectric prosthesis function [
8,
9,
10,
11]. By this approach the reinnervated muscles can act as biological amplifiers of motor commands in the amputated nerves, and the resultant surface EMG can be used to improve the myoelectric prosthesis control. The TMR is most useful for high level amputations (such as shoulder disarticulation amputation and short trans-humeral amputation in particular), which usually transfers amputated nerves to the pectoralis muscles for creation of additional myoelectric control sites. Thus the control signals measured over the reinnervated muscles near the heart are very likely to be corrupted by significant ECG interference, which can distort any EMG amplitude measurements for proportional myoelectric prosthesis control.
To reduce the influence of ECG interference, many methods have been developed to remove ECG artifacts from surface EMG signals [
3,
4,
5,
6,
7]. However, for the purpose of the real-time myoelectric prosthesis control, high pass filtering (through filters built in the head stage of recording electrodes or through digital signal processing) is routinely used in clinical practice. Depending on the signal characteristics of both the surface EMG and the ECG interference, the cut-off frequency of the high pass filtering can be set anywhere between 30 Hz and 100 Hz for effective removal of the ECG contamination. In spite of its convenient implementation, a major limitation of the high pass filtering is the unavoidable removal of useful surface EMG signals when filtering the ECG interference due to spectral overlap between both signals. Specifically, a relatively larger cut-off frequency has been suggested to reduce more ECG interference, and however, useful surface EMG components as well. The problem becomes more serious for female patients because the breast tissues between the reinnervated chest muscles and the surface electrode will further strengthen the volume conductor effect [
10]. As a result, the recorded surface EMG signals contain relatively more low-frequency components. Thus, increasing the cutoff frequency of high pass filters for ECG artifact removal will significantly suppress the useful surface EMG signals. To overcome this limitation, more complicated methods such as ECG template subtraction, adaptive filtering, wavelet thresholding, and independent component analysis (ICA) have been developed [
3,
4,
5,
6,
7]. While these methods can remove ECG artifacts with relatively small distortion of surface EMG signal, they have limitations that constrain their application in myoelectric control [
12]. For ECG template subtraction,
a priori information about the ECG waveform has to be obtained [
3]. For adaptive filtering, an extra channel is required to record the reference signal [
7]. The ICA based methods require simultaneous recording with a number of EMG channels [
4]. A relatively long delay may be imposed by the wavelet thresholding methods for ECG artifact removal [
5].
In this study, we propose a novel approach based on sample entropy (SampEn) analysis [
13,
14] to process surface EMG signals with different degrees of ECG interference. A practical and quantitative way of measuring complexity of a signal or a system generating that signal is the use of entropy [
13,
14], and the SampEn is a representative entropy measure suitable for analyzing nonstationary biomedical signals [
14]. Both EMG signals and ECG inteference can show different complexity characteristics due to their different electrophysiological origins. Thus, the two signals can be differentiated in the nonlinear complexity domain via SampEn analysis, although they are always overlapped in the conventional time and frequency domains. Our previous work reported that SampEn analysis was useful for EMG onset detection by highlighting EMG bursts while overcoming ECG interference [
15]. Istenic
et al. [
16] also found that the EMG complexity quantified by SampEn was correlated with muscle contraction level. Inspired by these findings, this study further demonstrated that the SampEn analysis can be used to reliably estimate the EMG signal intensity even in the presence of dramatic ECG contamination. Therefore, the SampEn analysis of surface EMG provides an useful approach to overcoming the effect of ECG artifacts. With advances in microprocessors for myoelectric prosthesis control, it is promising to use SampEn analysis as an alternative approach to implementing proportional myoelectric control, especially for high level amputee patients after the TMR surgery.
2. Methods
2.1. Experiments
The testing data for evaluation of the proposed SampEn analysis based method for proportional myoelectric control were derived from two experiments, performed with an able-bodied male subject (30 years old) and a shoulder disarticulation amputee subject after TMR, respectively. All experimental procedures were approved by the Institutional Review Board of Northwestern University (Chicago, IL, USA). Both subjects gave their informed consent before participating in the study. The surface EMG signals were recorded using a 128-channel Refa EMG system (TMSi, Oldenzaal, The Netherlands). The reference electrode was located on the bone area of the elbow and for each channel the system had a common feedback subtraction of the average of all the recording channels. The size of each individual recording electrode was 5 mm in diameter. For each channel, the signal was sampled at 2000 Hz with a band pass filter set at 20–500 Hz.
For the able-bodied subject, a grid of 24 surface electrodes, arranged in a 3 × 8 formation, was placed around the forearm muscles, and the surface EMG signals were recorded while the subject sequentially performed 10 repetitions of isometric contraction of hand grasp. Each contraction was maintained for 3 s and followed by a brief rest period of 5 s. For each repetition, the subject was asked to exert a comfortable consistent level of contraction. Additionally, the subject was asked to gradually increase the contraction level from low to high, in order to produce surface EMG signals across different intensities during a ramp contraction. The purpose of recording from the forearm of an able-bodied subject was to obtain a “clean” surface EMG dataset free of ECG interference which can be used to generate semi-synthetic surface EMG signals with ECG contamination.
The TMR subject was a 54 year old man with bilateral shoulder disarticulation amputation, who was the first TMR surgery subject in the world [
8]. The TMR procedure in this subject was that the pectoralis muscles were denervated, and then four brachial plexus nerve transfers were performed (on the left side). Three arm nerves were transferred to three segments (upper, middle and lower) of the pectoralis major muscle. The ulnar nerve was transferred to the pectoralis minor muscle on the lateral chest wall. Surface EMG signals were recorded from the TMR subject with surface electrodes placed over the nerve transfer sites of the reinnervated pectoralis muscles, during the subject’s imagining and actuating different movements (e.g., hand open, hand close, wrist supination, wrist pronation,
etc.) involving the missing limb. The protocol was similar to that reported in our previous study [
9]. Repetitions of each movement were performed. In each repetition of the movement, the subject was asked to perform isometric muscle contraction at a comfortable and stable level for approximately 5 s, and then rest for 5 s before the next contraction started. The ECG signals during the rest period were selected in this study as “pure” ECG interference dataset, in order to generate semi-synthetic surface EMG signals with ECG contamination.
2.2. Semi-synthetic Testing Dataset Generation
Surface EMG data recorded from the forearm of the able-bodied subject was free from ECG interference due to the large distance from the heart to each electrode. Such “clean” EMG data was used to be artificially corrupted by “pure” ECG interference recorded from the pectoralis muscles of the TMR subject during the rest period. Thus a group of semi-synthetic surface EMG signal segments was derived, which can be used to quantitatively evaluate the performance of the proposed SampEn based method for proportional myoelectric control in the presence of different degrees of ECG interference. In more details, five segments of background ECG noise, with different QRS complex shapes (at different channels) and intervals (over different time durations), were first selected from the dataset of “pure” ECG interference. Each segment was a single channel recording of ECG interference for 5 s. Meanwhile, from the “clean” surface EMG dataset, another 10 segments of EMG activity recorded during voluntary muscle contractions were selected. For the multiple channel recordings, the channel demonstrating the highest overall EMG intensity/amplitude was used in this study. Each segment of the EMG activity corresponded to one of ten isometric contractions, with 2 s data selected from the 3 s contraction period. Then, the 10 “clean” surface EMG segments were scaled over a range of magnitudes, and summed with each of the five pure ECG interference segments (starting from 2 s to 4 s in the entire 5 s period) respectively. The scale of the “clean” surface EMG segment was quantified by signal-to-noise ratio (SNR) for the signal generated by the combination of the scaled “clean” surface EMG segment and a “pure” ECG interference segment. In order to investigate the effect of varying levels of surface EMG activity, six different SNRs of −10, −5, −2, 0, 2, 5 dB was used respectively for scaling original “clean” surface EMG activity. Consequently, 300 segments (10 “clean” EMG segments × 5 “pure” ECG segments × 6 SNR levels) of semi-synthetic surface EMG signals with ECG interference were generated in total. These semi-synthetic surface EMG signals with ECG contamination were formed, in order to quantitatively evaluate the performance of the proposed SampEn based approach for myoelectric proportional control in the presence of different degrees of ECG interference.
In addition to scaling the “clean” surface EMG segments to simulate different levels of ECG contamination, a combination of the “clean” surface EMG signals from the ramp contraction of the able-bodied subject and the “pure” ECG interference was also generated. The signal was processed with the SampEn analysis to qualitatively demonstrate the effectiveness of the proposed method for overcoming ECG interference, thus facilitating proportional myoelectric control.
2.3. Signal Processing
In order to estimate EMG intensity for the purpose of proportional control, the myoelectric input is usually divided into a series of overlapping analysis windows. A larger window length contains more data samples toward more reliable estimate of EMG signal intensity, but leads to larger signal processing delay. Considering the tradeoff between the performance and the imposed processing delay, the analysis window length was determined to be 200 ms and the window increment was 8 ms in this study. Subsequently, the SampEn analysis was performed on each analysis window, as described below.
Entropy is a statistical measure of irregularity or complexity of a dynamic system [
13,
14]. The calculation of entropy is based on a time series generated from the system to be quantified. Among many different algorithms for calculating the entropy, the approximate entropy (ApEn) [
13] and the sample entropy (SampEn) [
14] are widely used in biomedical signal processing [
15,
17,
18]. The SampEn can be considered as a refinement of the ApEn to reduce the bias caused by self-matching [
14], thereby demonstrating relative independence of recording length. The SampEn was used in this study because of its strength for robust complexity measure of short and noisy time series. A brief summary of the SampEn calculation is presented here, with a slight modification from its original description by Richman and Moorman [
14].
To calculate the SampEn of a time series
,
, in the delayed
m-dimensional space, a number (
) of vectors are first constructed as:
A pair of two such vectors,
and
are defined to be similar if:
where
r is a predefined tolerance. Then, let
be the number of vectors
that are similar to
, where
j ranges from 1 to
and
to exclude self-matching. In this case,
is defined as
. Next,
is further defined to be:
Similarly, for the (
m+1)-dimensional space,
can also be defined as
times the number of vectors
that are similar to
, where
j ranges from 1 to
(
), and set:
Last, SampEn is computed as:
The input parameters, both dimension
m and tolerance
r, need to be determined for the SampEn calculation. Some existing rules have been reported in various applications of the SampEn analysis in processing biomedical signals, generally suggesting the use of
m to be 2 and tolerance
r between 0.1 and 0.25 times standard deviation (SD) of the processed time series [
13,
14,
15,
17], while a larger tolerance is suitable for signals with short duration [
14]. It is also suggested that the use of a uniform/fixed tolerance applied to all analysis windows facilitates the quantification of instantaneous change in signal complexity across windows [
14,
15], which is crucial for proportional control. Thus in this study the tolerance
r was roughly estimated and globally preset to be 0.25 times SD of the signal segments to be processed.
2.4. Performance Evaluation
For performance comparison, the root mean square (RMS) was also calculated for each analysis window. The RMS amplitude is an appropriate EMG parameter for estimating muscle force, which has been widely used in proportional myoelectric control [
1,
2]. Since high pass filtering methods are routinely used in clinical practice to remove ECG interferences from myoelectric control signals, a fourth-order Butterworth filter with different cut-off frequencies of 30, 40, 60 and 100 Hz, respectively, was also implemented. The effect of high pass filtering on ECG interference removal and RMS amplitude calculation was compared with the SampEn-based method. For the semi-synthetic surface EMG signals that was artificially corrupted by ECG interference, the RMS amplitudes of the original “clean” surface EMG signals with different intensities (before adding ECG interference) were also calculated. Thus, the performance of different methods was simply assessed by the correlation coefficient
R between the RMS of the “clean” surface EMG signal and the processing results obtained from each of the methods. The two-way repeated-measure analysis of variance (ANOVA) was applied on the correlation coefficient
R, with the signal processing method (5 levels: high-pass filtering with 30, 40, 60 and 100 Hz cut-off frequencies and the SampEn method) and the SNR level (6 levels: −10, −5, −2, 0, 2 and 5 dB) both considered as within-subject factors. The level of statistical significance was set to
p < 0.05 for the ANOVA.
In order to evaluate the proportional control capability of the proposed SampEn-based method, regression analyses were conducted to further construct the relation between the SampEn of the artificially ECG corrupted EMG signals and the RMS amplitude of the corresponding “clean” surface EMG signals.
3. Results
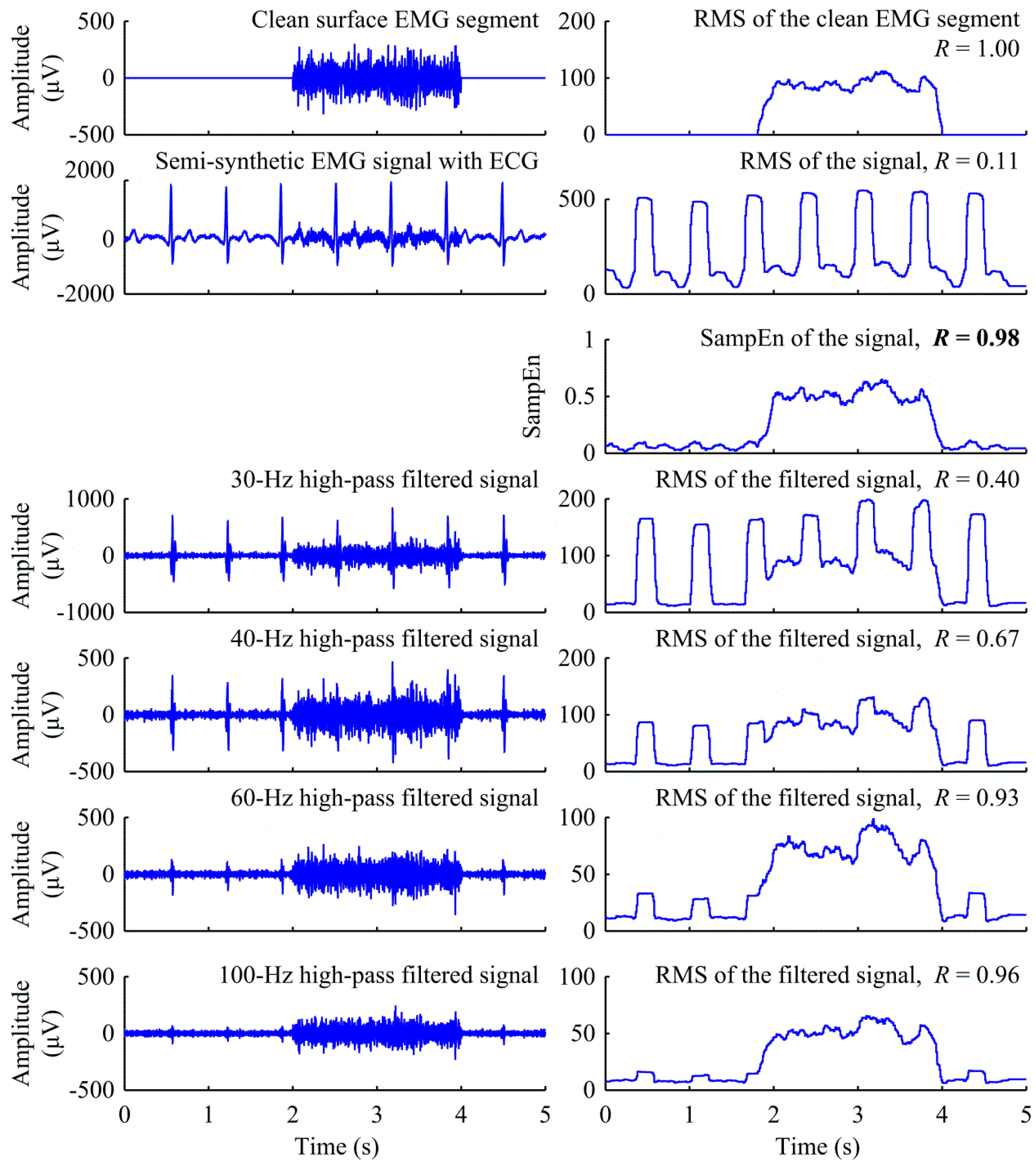
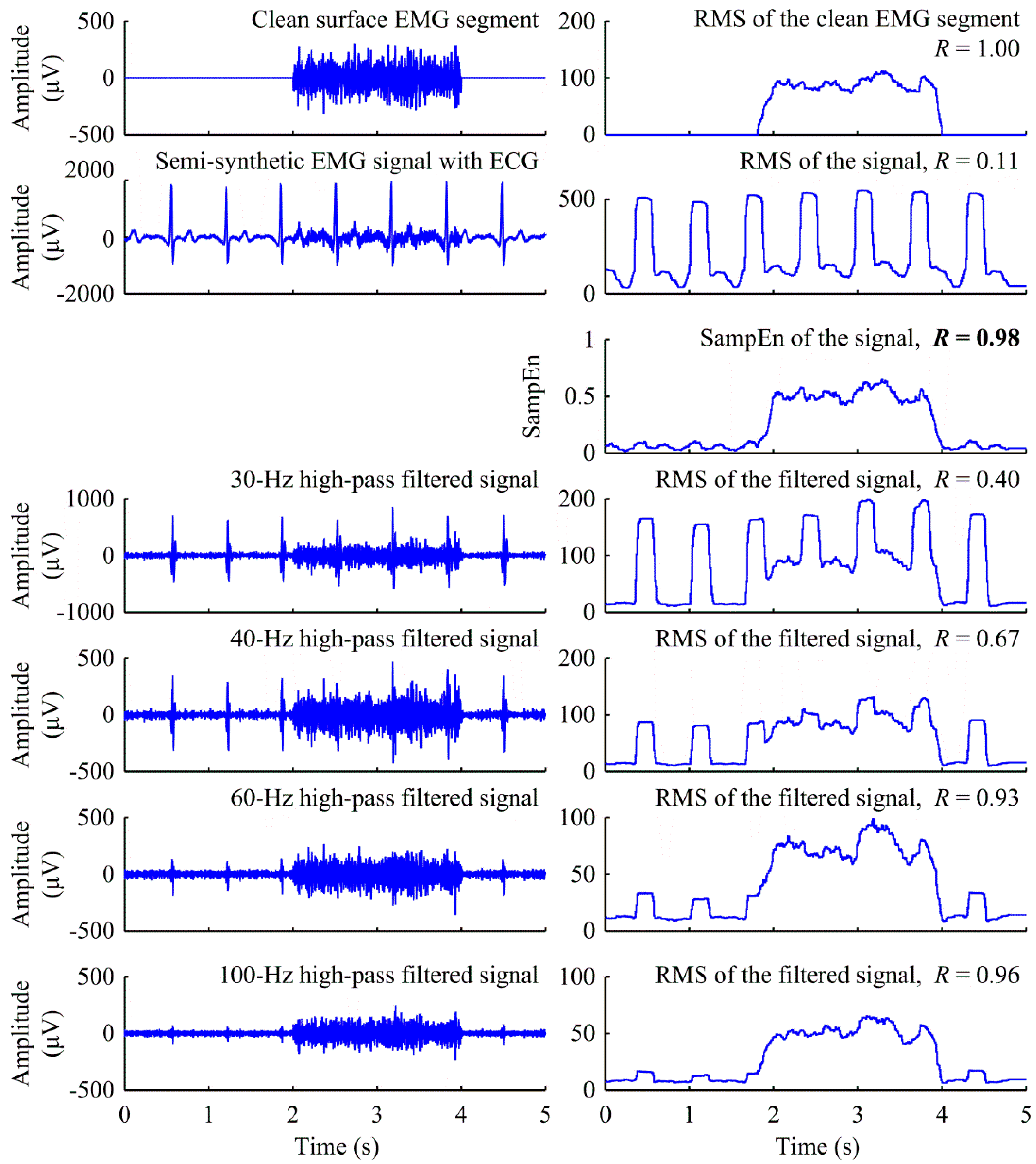
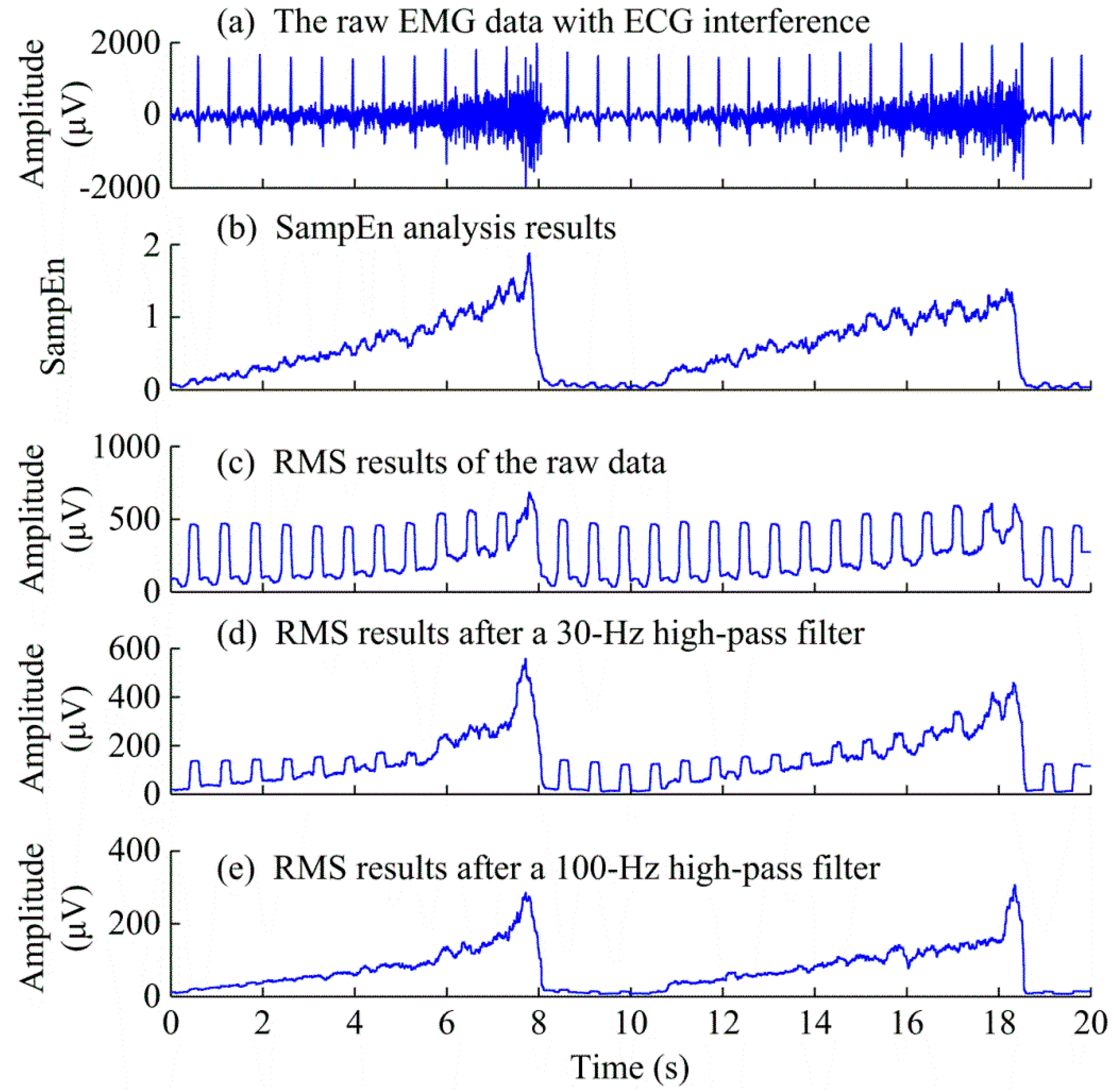
Figure 1 is a representative illustration of the semi-synthetic surface EMG signal processing in the presence of dramatic ECG interference, using the SampEn based method and the high pass filtering with different cut-off frequencies, respectively. First, it is observed from this figure that for the raw surface EMG, the RMS amplitude of the signal had steep oscillations due to the presence of significant ECG interference, resulting in a very low correlation coefficient with respect to the “clean” surface EMG signal (
R = 0.11). It was found that suppression of the ECG interference in the surface EMG signal was achieved using high-pass filtering. In this example, when the cut-off frequency of high pass filtering was set to be 30 Hz, the majority of the ECG interference still remained in the signal. This resulted in an increased but still low correlation coefficient between the “clean” surface EMG and the filtered signal (
R = 0.40). When the cut-off frequency of high pass filtering was increased to 40 Hz, 60 Hz and 100 Hz respectively, more and more ECG interference was removed from surface EMG. However, the ECG interference was still discernible even for the 100 Hz cut-off frequency. Meanwhile, more and more useful EMG components were also removed as demonstrated by the reduced RMS amplitude with increase of the cut-off frequency (
Figure 1). The correlation coefficient between the RMS of the “clean” surface EMG signal and the high-pass filtered results improved to 0.67, 0.93, and 0.96 when the cut-off frequency was set to be 40 Hz, 60 Hz and 100 Hz, respectively.
By contrast,
Figure 1 also shows the performance of the SampEn-based method for overcoming the effect of ECG interference toward estimation of surface EMG intensity. It was observed that the ECG interference was largely suppressed in the SampEn domain, and the SampEn curve closely tracked the RMS amplitude curve of the “clean” surface EMG signal, demonstrated as a high correlation coefficient between the two signals (
R = 0.98).
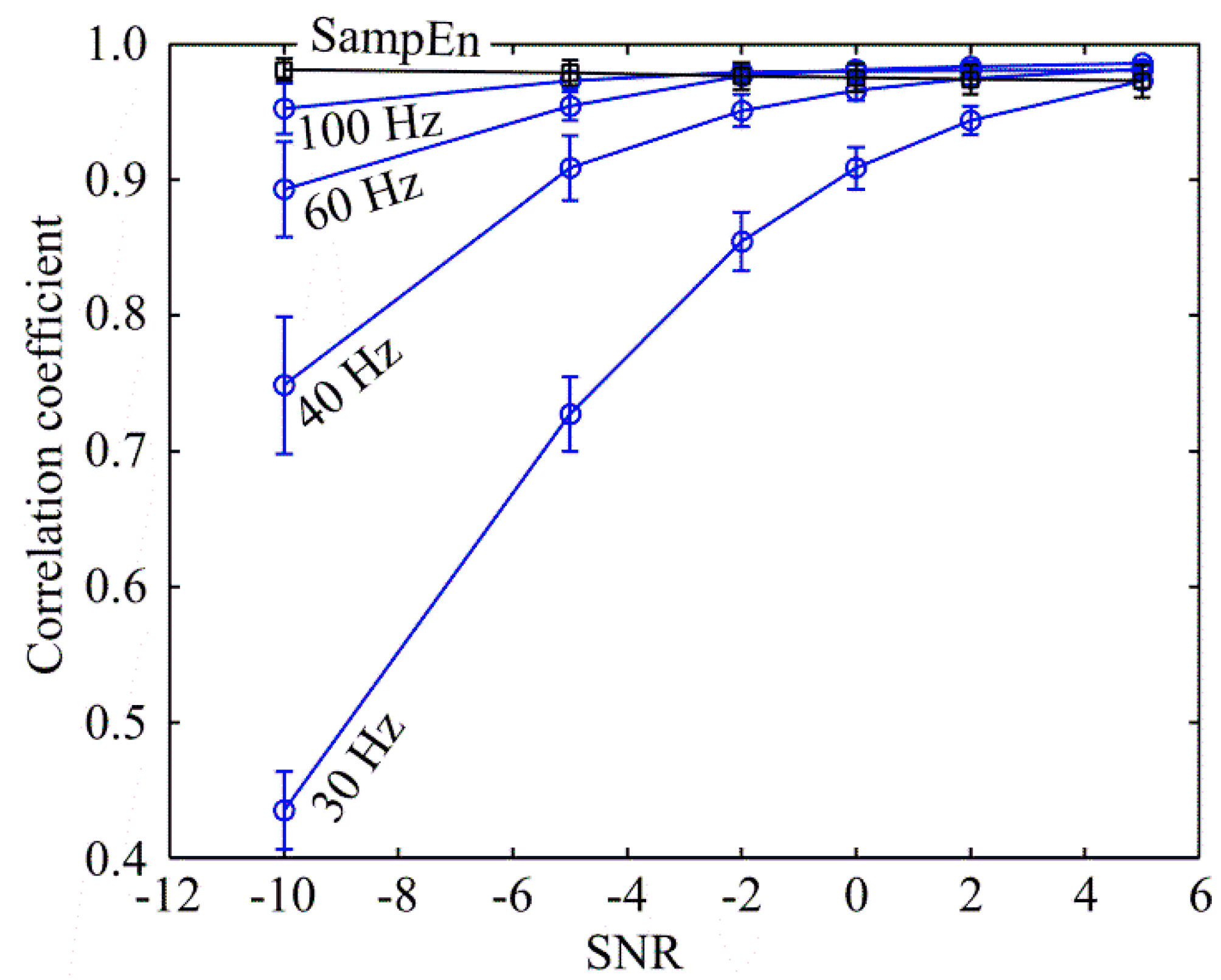
Figure 2 reports the performance of both the conventional high-pass filtering method and the proposed SampEn method for proportional control variable estimation under the presence of ECG interference, as described by the correlation coefficient
R averaged across all 50 semi-synthetic signal segments (10 “clean” EMG segments × 5 “pure” ECG segments at each SNR level). It can be observed that the performance of the high-pass filtering method was dramatically decreased when the SNR level was relatively low, and the most severely affected performance appeared at the use of the lowest cut-off frequency (30 Hz). By contrast, the SampEn method achieved relatively stable performance across different SNR levels. At low SNR levels, the SampEn method was able to outperform all high-pass filtering methods, with statistical significance (
p < 0.001) revealed by the two-way repeated-measure ANOVA, while the performance of both the SampEn method and the 100 Hz high-pass filtering method were comparable at higher SNR levels. In addition, the performance of the SampEn method was even found to show a slight decreasing trend when the SNR was increased, leading to a lower mean correlation coefficient than that of the 100 Hz high-pass filtering method at the SNR of 5 dB, also with statistical significance (
p < 0.05).
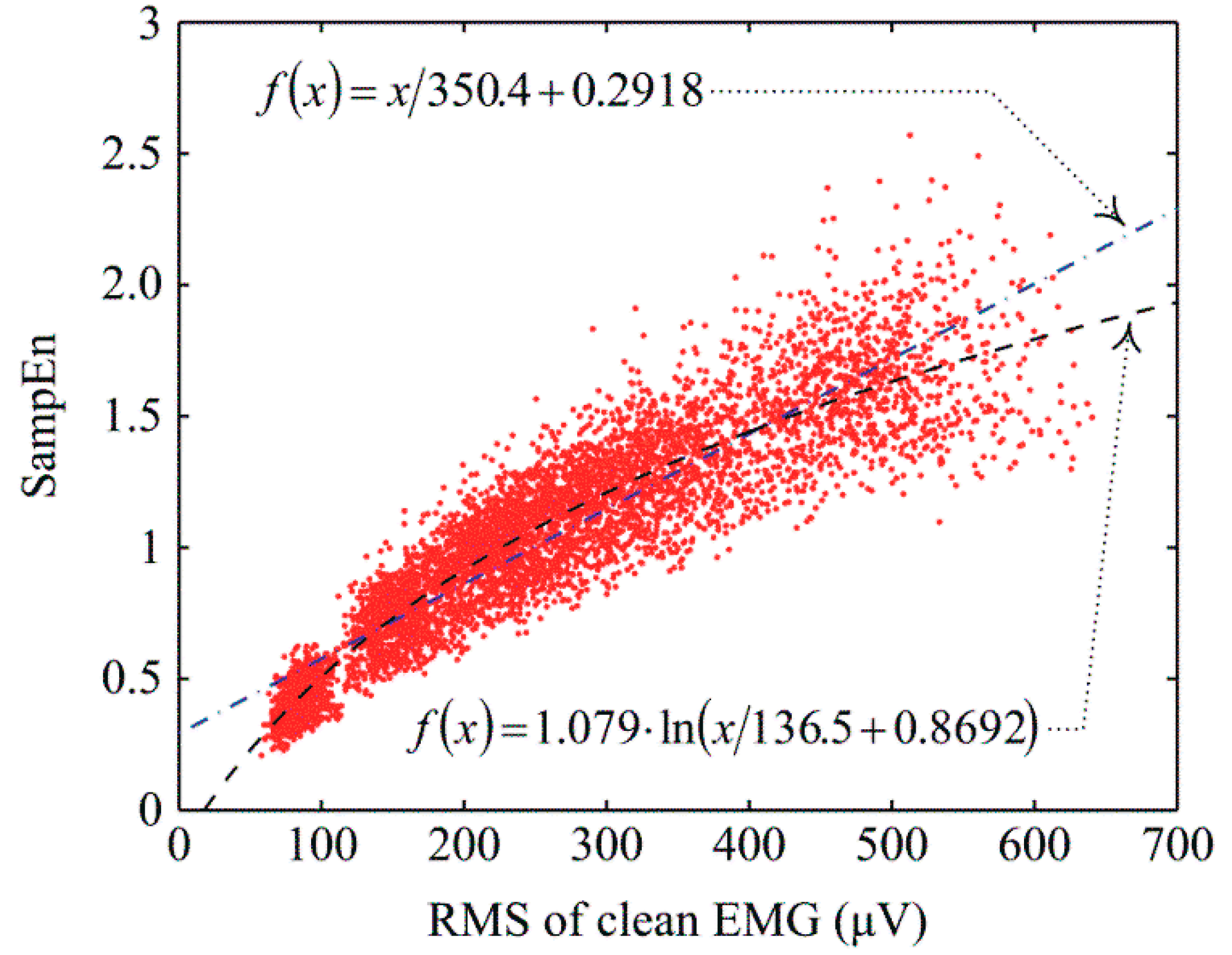
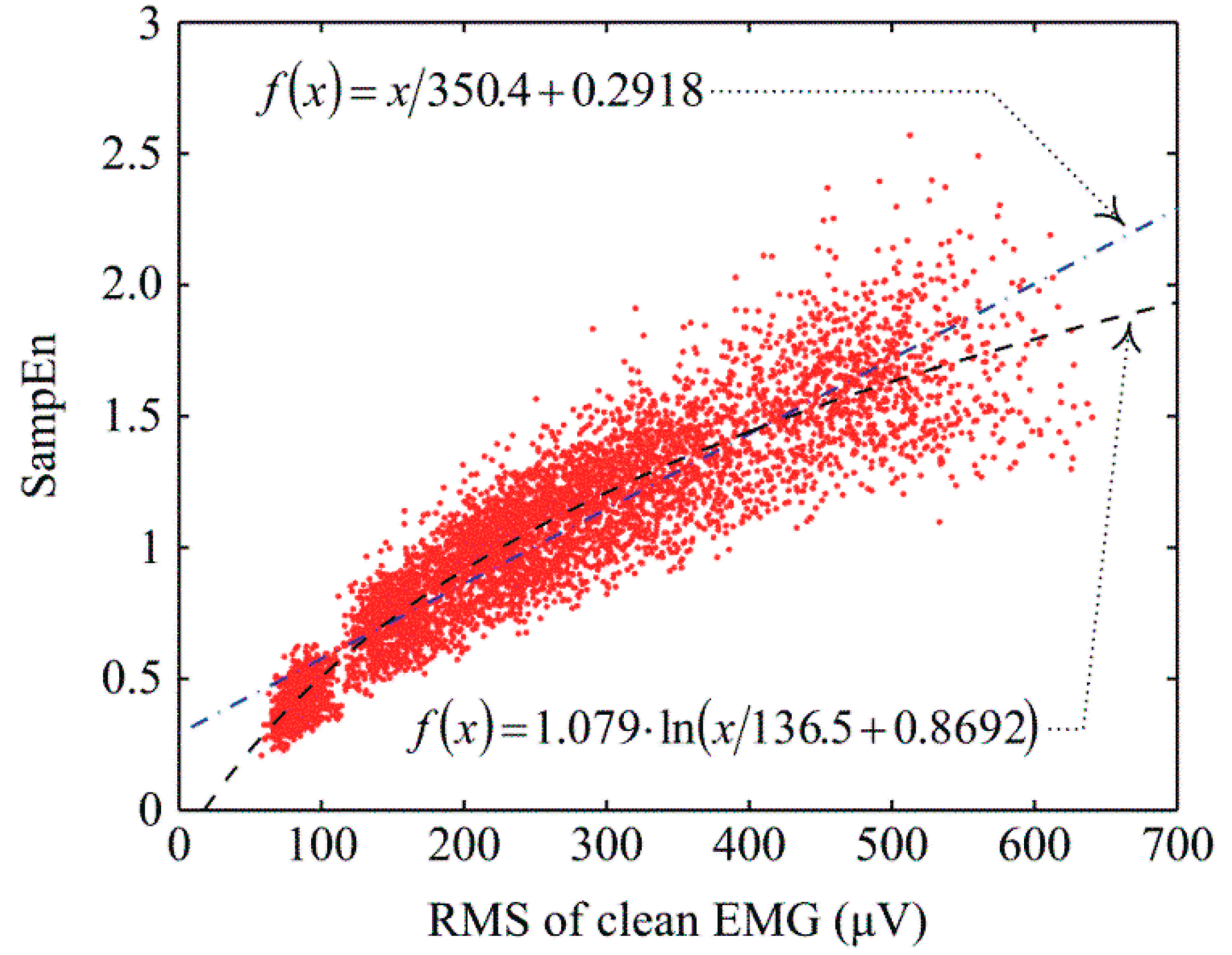
Figure 3 plots the RMS amplitude of the “clean” surface EMG signals
versus the corresponding SampEn values of their ECG corrupted signals. The points in the figure were derived from all the analysis windows during the periods of voluntary muscle contraction (
i.e. the period from 2 s to 4 s within each segment of the semi-synthetic signals). A strong positive correlation between the RMS amplitude (of the “clean” surface EMG signal) and the SampEn value (of the ECG-corrupted surface EMG signal) was observed. A linear regression was first conducted to test the linearity of the relation. It was found that a linear function
fitted all the data points with a norm-of-residuals value of 13.1 and an
R-squared value of 0.83. As demonstrated in
Figure 3, a linear fitting was not able to characterize the relation well at lower levels of EMG intensity (RMS amplitude less than 100 µV). Therefore, the relation was fitted by a different function
. With this logarithmic fitting, the norm-of-residuals value was improved to 11.8 and the
R-squared value increased to 0.86, suggesting that the logarithmic function better described the examined relation.
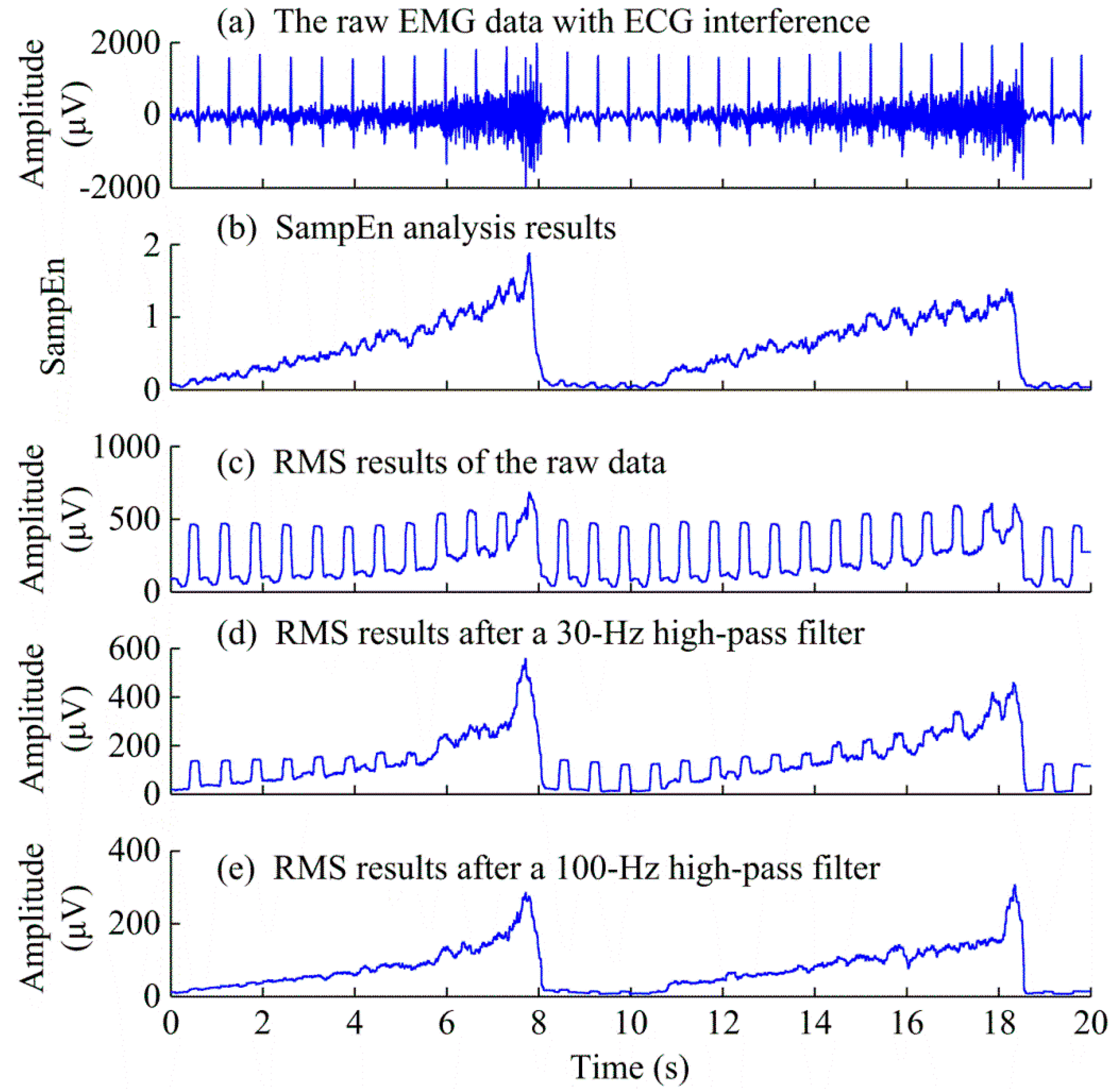
Figure 4 shows the processing results of a surface EMG signal in the presence of dramatic ECG interference during gradual increase of the contraction level, using the SampEn based method and the high pass filtering with different cut-off frequencies, respectively.
It was observed that compared with high-pass filtering methods, the resultant SampEn curve exhibited a robust performance to overcome the effect of ECG artifact and track the intensity changes of the surface EMG signal.
4. Discussion
This study can be considered as a follow-up one based on our previous efforts [
15,
19], which addressed the ECG interference in EMG onset detection by applying the SampEn analysis. In this paper, a novel and extensive application of the same SampEn analysis is presented for overcoming the influence of ECG interference on EMG intensity estimation, with the view toward better implementation of proportional myoelectric control, especially for prosthesis users whose pectoralis muscles are often involved in the TMR procedure to create additional myoelectric control sites.
The neuromuscular system is a nonlinear dynamic system with EMG and force being its electrical and mechanical outcomes, respectively [
18]. As compared with EMG signals, ECG interference is derived from a different electrophysiological process demonstrating different complexity characteristics. Thus the two signals can be differentiated in the nonlinear dynamic domain to suppress the effect of ECG artifacts on EMG signal processing, as representatively shown in
Figure 1 and
Figure 4b. Furthermore, the increase of muscle force requires recruitment of more motor units and/or increase of their firing rates. This process is accompanied by a complexity increase of the resultant EMG [
16]. Thus it is feasible to use nonlinear dynamic parameters such as the SampEn measurement to minimize the effect of ECG interference (without removing it) and meanwhile track the surface EMG intensity changes toward proportional myoelectric control. This was demonstrated by the strong correlation between the resultant SampEn values and the amplitude measurements of the “clean” surface EMG signals in the presence of significant ECG interference, as shown in
Figure 3. By contrast, with cut-off frequency increased from 30 Hz to 100 Hz, high pass filtering reduced more and more ECG interference, and useful surface EMG components as well, therefore yielding decreased RMS amplitude of the filtered signal shown in
Figure 1. Dramatic attenuation of useful surface EMG signals by high-pass filtering can also be found in the representative example in
Figure 4. By qualitative analysis, the 100 Hz high-pass filter cannot produce smooth RMS results in proportion to gradually increased EMG intensity, for the later repetition in particular. This indicated that using high-pass filtering to remove ECG interference with unavoidable attenuation of EMG components might lead to poorer proportional control performance, when compared with direct EMG intensity estimation regardless of the ECG by the SampEn method.
The method based on SampEn analysis does not require extra EMG channel recording or a priori information about the ECG template. Indeed, the EMG intensity estimated using the SampEn analysis is not sensitive to changes in ECG features (e.g., amplitude, duration and shape) and SNR levels. The sliding window approach for calculating the SampEn is suitable for real time implementation. The requirement of presented and globally fixed input parameters (both dimension m and tolerance r) also facilitates SampEn calculation in real time. Because of these advantages, the SampEn analysis can provide a convenient approach for reliable and robust estimation of muscle intensity in the presence of different degrees or forms of ECG interference.
It should be acknowledged that compared with amplitude measurement, the SampEn-based method imposes more computational burden due to the complexity of the SampEn calculation. In our computational platform with a processor at 3.3 GHz (Intel Core i3-3220) and 4 GB RAM running a customized program in a Matlab environment (version 2012, The Mathworks Inc., Natick, MA, USA), it took almost 50 ms to compute a SampEn value for each 200 ms analysis window, as compared with no more than 1 ms for an amplitude calculation. Although optimizations in computational methodology, such as multi-threading and parallel computing, may further reduce the time delay, future advances in microprocessors need to be considered in the development of any real time myoelectric control system using the SampEn based method. In addition, as demonstrated in
Figure 3, the results with semi-synthetic data reveal a nonlinear logarithmic relationship between SampEn and signal intensity (RMS) of the surface EMG signals. For practical implementation of myoelectric proportional control, further calibration is needed with respect to how to best map the control variable (SampEn) to output prosthesis variables (e.g., force, speed). Such procedures may be user or task specific. With this regard, the recruitment of only two subjects, one able-bodied subject to produce “clean” myoelectric control signals and one TMR subject for offering true ECG interference, remains another limitation for our current study. Many more prosthetic users after the TMR procedure need to be recruited for evolution of the proposed SampEn method toward practical application of proportional myoelectric control. Moreover, this study primarily focused on the methodological solution to myoelectric proportional control in the presence of significant ECG interference. Beside the off-line data analysis, real-time implementation of proportional control is required to evaluate the controllability of the proposed SampEn approach and its advances with respect to the conventional high-pass filtering method. All these remain our future work.
In addition, this study focuses on myoelectric prosthesis control for amputee subjects, especially for patients with TMR surgery. Surface EMG can also be as a control signal for assistive training devices toward neurologic injury rehabilitation. For neurologic injury (such as hemiparetic stroke) patients, voluntary surface EMG signal is sometimes accompanied by spontaneous motor unit activity recorded as slowly firing tonic spikes [
20]. Removal of such spontaneous spikes from voluntary surface EMG is a difficult task because of their same physiological origins (muscle fibers). Due to different complexity characteristics of spontaneous and voluntary surface EMG signals, the SampEn analysis can also be useful to suppress spontaneous spikes for surface EMG signal processing [
15]. In this regard, the presented approach in this paper might be extensively applied to myoelectric proportional control of rehabilitative devices designed for patients with neurological injury.
Finally, this study investigates a method to overcome the effect of ECG interference toward implementation of proportional myoelectric control. It is worth noting that myoelectric pattern recognition based control is a more advanced control strategy that relies on feature extraction and classification analyses of surface EMG signals to identify the movement intention [
21]. The effect of ECG interference on the classification accuracy of surface EMG signals was examined in a previous study, and it was found that the ECG interference had little effect on the classification accuracy [
22]. A recent study with neurological injury patients also revealed that presence of involuntary EMG interference in both the training and testing datasets would not compromise myoelectric pattern recognition performance [
23]. These findings suggest that while ECG or other artifacts (such as spontaneous EMG) should be removed to implement a proportional myoelectric control system, it is not necessarily imperative to suppress these artifacts that contaminate voluntary surface EMG signals for implementation of a myoelectric pattern recognition based system. Thus, the ECG interference should be appropriately addressed according to the design of a myoelectric control system.



{kind=link}
{kind=link}
{kind=link}
{kind=link}